
How anti-LGBTQ+ medical disinformation is generated and used to influence policy.
Opponents of gender-affirming care for minors centrally claim that they are following common sense, sound scientific principles and medical ethics. They argue that medical systems have been ideologically captured and deceived into supporting gender-affirming care on the basis of dubious evidence.[1]
To say ‘the science is settled’ on the medical effectiveness of gender-affirming care is intellectual dishonesty at best, and medical malpractice at worse. Given the permanency of puberty blockers, cross-sex hormones, and gender reassignment surgeries, there is not enough reliable evidence for doctors or parents to make informed decisions in favor of these practices, and children simply do not have the capacity of consent.”
– Tennessee State Sen. Jack Johnson (R-TN), sponsor of SB 1 banning gender-affirming care for Tennessean trans youth, defends his bill in an op-ed for The Tennessean, Feb 13, 2023.
The overarching strategy employed here relies upon an ecosystem of think tanks, legislators, political candidates, public intellectuals and gender-critical bloggers (described in greater detail in Chapter 5), which advances a position against gender-affirming care by manufacturing plausible deniability regarding evidence in favor of said care. Rather than spreading outright falsehoods per se, they misrepresent existing scientific evidence, omit key context, and selectively apply critical standards in order to argue that youth seeking gender-affirming care will in reality be harmed by this care, rather than benefit from it. At its most sophisticated, this strategy does not even need to argue against the idea that some youth are transgender and will benefit from care — only to argue that scientific consensus is lacking and that the broader evidence base precludes certainty, thereby justifying stringent gatekeeping requirements.
At all levels, however, the key is manufacturing doubt — creating sufficient uncertainty about potential risks and arguing that this uncertainty renders providing gender-affirming care unethical. Manufactured doubt is not uncommon in publicized, politicized debates with scientific stakes.[2]
Conservative think tanks like the Heritage Foundation, the Competitive Enterprise Institute and the George C. Marshall Institute are old hands at this strategy. They have routinely elevated ostensible experts to either deny anthropogenic climate change, or (at minimum) claim that there “is no consensus” among scientists on this matter.[3] The Heritage Foundation — an instrumental, historical mainstay in shaping American conservative policy — in particular has supported groups through funding and hosting forums advocating similar strategies to justify denying adoption rights to queer parents, to justify opposition to same-sex marriage, to problematize the use of hormonal birth control, and to oppose COVID-19 prevention measures and vaccination mandates, as well as gender-affirming care for anyone, much less minors.
The Left accuses Republicans of creating this new fight in the culture wars out of whole cloth. In reality, we’re simply responding to a rapid onset of transgender ideology being pushed on our children in their schools, libraries, and even doctors’ offices. This is an entirely new phenomenon, pushed by people who know better in pursuit of so-called ‘compassion’ for children suffering from sometimes temporary ideations about their gender.”
– U.S. Rep. Dan Crenshaw (R-TX), who sponsored a bill to bar federal funding to Texan hospitals that provide gender- affirming care to trans youth, writes in an op-ed for Newsweek, Aug. 31, 2023.
Thus, it is little surprise that religiously motivated conservative think tanks are adapting and expanding their playbook to target gender-affirming care for minors. Not only does the Heritage Foundation explicitly decry the “toxic normalization of transgenderism” as a critical issue facing the nation in its Project 2025 agenda, one of the coalition partners of that agenda is the organization that has spearheaded not only the draft legislation for gender-affirming care bans but has been their key defensive litigant in court challenges — the Alliance Defending Freedom (ADF), a hate group with a long record of anti-LGBTQ+ legislative and judicial activism.
They are hardly alone in this matter: Leaked documents[4] reveal that they have worked hand-in-hand with the American College of Pediatricians (ACPeds), an anti-LGBTQ+ pseudoscience organization that split from the American Academy of Pediatrics (AAP) in 2002 over the AAP’s support for LGBTQ+ parents to adopt children,[5] has worked extensively with the ADF to provide evidence for “Vulnerable Child Protection Acts.” As early as 2014, ADF explicitly solicited white papers from ACPeds (even offering a $15,000 grant in the process), hoping to “substantiate” ADF’s ideological positions on “transgender/gender identity issues,” dictating positions that the white paper would take (e.g., “Substantiate that it is normal during adolescence for children to go through a phase when they identify (to some degree) with the opposite sex”).[6]
South Dakota state Rep. Fred Deutsch, who filed the “test balloon” HB 1057 banning gender-affirming care for trans youth in 2020,[7] relied on such a document created and distributed within a secret working group including multiple ACPeds members (Andre Van Mol, Michelle Cretella and Michael K. Laidlaw), as well as representatives from other conservative groups (e.g., Family Policy Alliance and Eagle Forum), and founders of the then-nascent Society for Evidence-Based Gender Medicine (SEGM).[8] As originally reported by Mother Jones, this secret working group was instrumental in launching the ongoing wave of anti-transgender legislation.[9] One member of this group — Vernadette Broyles of Child & Parental Rights Campaign, an anti-LGBTQ+ Christian Right legal firm now challenging trans-inclusive school policies in Massachusetts — soon put together a legislative packet with a generic white paper based on the original paper written for South Dakota. That legislative packet was intended “to be used in support of the Vulnerable Child Protection Acts being introduced in our respective states,” according to a January 2020 email to the working group.
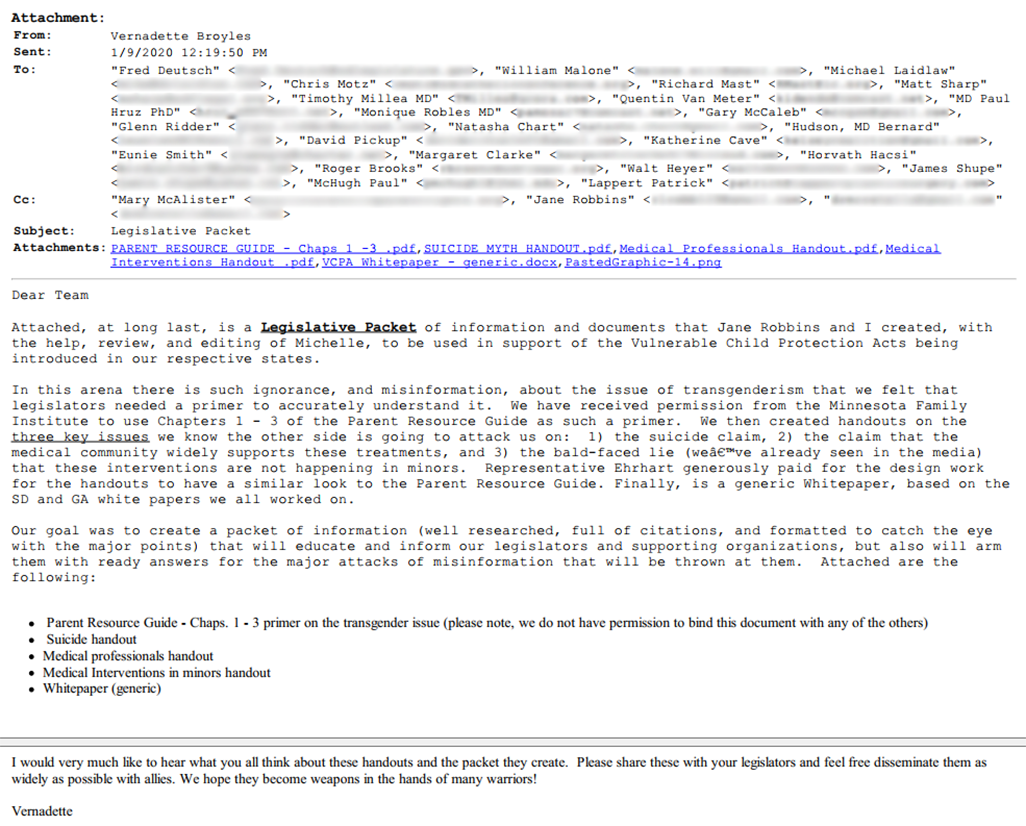
Figure 4.1: Vernadette Broyles of Child & Parental Rights Campaign emailing the secret working group covered by Mother Jones on Jan. 9, 2020. She shares a collection of resources to the group, including a legislative packet and a generic white paper, to push the anti-trans model bill Vulnerable Child Protection Act throughout the country.
Andre Van Mol sent a similar resource document to the Florida Agency for Health Care Administration (AHCA) as the agency sought to draft a rule blocking Medicaid coverage for gender-affirming care.[10] The rule was later challenged in the case Dekker v. Weida, and the judge ruled it was unconstitutional and based in politics, not science or medicine.[11] Researcher Zinnia Jones noticed significant overlap between the file submitted to Florida AHCA and a document titled “Opus,” housed on the exposed ACPeds Google Drive and ostensibly authored by Andre Van Mol.[12] Recently, ACPeds has begun hosting resource packets presenting similar arguments using similar citations on a hosted website they call Biological Integrity, explicitly targeting a lay audience[13] as well as policymakers.[14]
These white papers’ explicit purpose is to manufacture justification for banning gender-affirming care (or at minimum, denying Medicaid coverage of gender-affirming care) that will be plausibly defensible in court, as these bills are swiftly challenged wherever and whenever they are signed into law. As a knock-on effect, these same organizations are empowered to challenge existing pro-trans legislation (e.g., conversion therapy bans).
In September 2023, Molly Redden of Huffington Post published a detailed report, complete with individual profiles of the small stable of well-compensated expert witnesses across cases involving gender-affirming care bans, the claims they typically make on-record, and why many of these claims are (at best) misleading.[15] She also documents the transparent bias many of the groups that these witnesses come from represent. This chapter will not reiterate an exhaustive profile of experts while one already exists; rather, the current chapter investigates how the strategies used by these groups function and overlap, and the associations between not only the groups themselves, but the information they rely upon, and to what degree these strategies are effective at defending gender-affirming care bans.
Methodology
We compiled anti-LGBTQ+ expert reports or declarations and legal complaint files filed in four high-profile, well-covered, relatively long-running cases pertaining to gender-affirming care and related issues: Eknes-Tucker v. Ivey, now Boe v. Marshall;[16] Kadel v. Folwell; Dekker v. Weida, previously Dekker v. Marstiller; and Tingley v. Ferguson (see Table 4.1). At present, many of these cases have had initial rulings in place blocking state laws banning care from going into effect, yet of these, Eknes-Tucker v. Ivey had its initial injunction against the state’s ban on gender-affirming care for trans youth reversed by the 11th Circuit Court of Appeals.[17] The 11th Circuit relied heavily on a recent order from the 6th Circuit in Tennessee that granted an emergency stay on an injunction for a similar ban, and the controversial Supreme Court decision overriding the right to abortion access guaranteed in Roe v. Wade.[18] As such, all of these cases remain ongoing and remain of public interest.
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r=0;r<e.length;r++)if(e[r].contentWindow===a.source){var i=a.data[“datawrapper-height”][t]+”px”;e[r].style.height=i}}}))}();
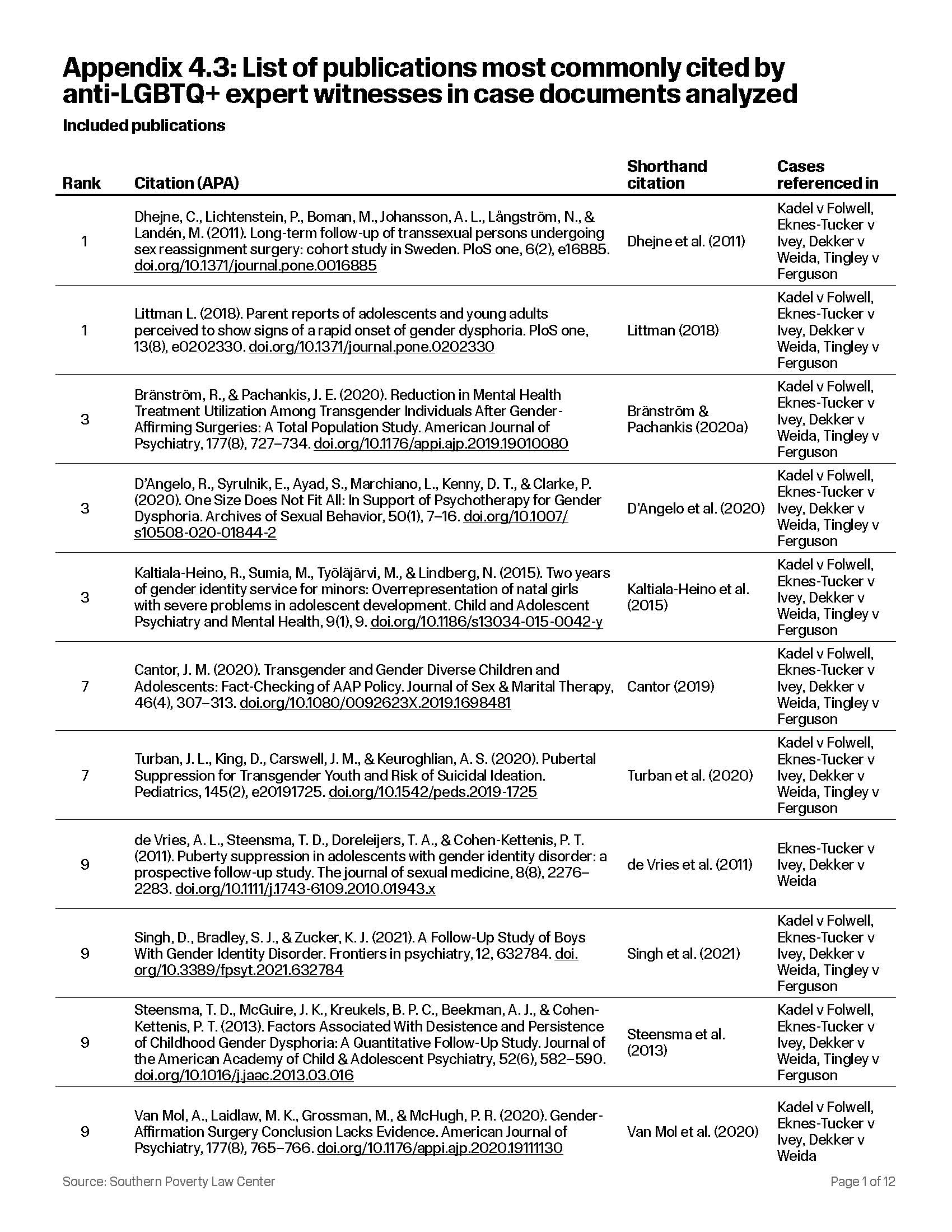
We noted and recorded all citations of academic publications from references, footnotes and in-body citations used in 29 expert declarations/reports from 16 groups or individuals submitted either to defend anti-LGBTQ+ policy (Kadel v. Folwell, Eknes-Tucker v. Ivey, Dekker v. Weida) or to challenge pro-LGBTQ+ policy (Tingley v. Ferguson) (Table 4.2). As Tingley v. Ferguson only included two anti-LGBTQ+ expert witnesses, one of the documents we reviewed was the initial complaint filed by Alliance Defending Freedom to get a more complete picture of the evidence base used for the case (see Appendix 4.1 for full list of reviewed documents).[19]
!function(){“use strict”;window.addEventListener(“message”,(function(a){if(void 0!==a.data[“datawrapper-height”]){var e=document.querySelectorAll(“iframe”);for(var t in a.data[“datawrapper-height”])for(var r=0;r<e.length;r++)if(e[r].contentWindow===a.source){var i=a.data[“datawrapper-height”][t]+”px”;e[r].style.height=i}}}))}();
Citation patterns were then mapped to visualize who most consistently used which papers. With the expert witnesses themselves representing one set of nodes (n=14)[20], or points of connection, and the documents they referenced comprising another (n=114), we identified 539 unique citations (defined as once per document) across all four analyzed cases (Figure 4.2). Nodes are sized based on the number of unique citations.
The Citation Network and Manufacturing Doubt
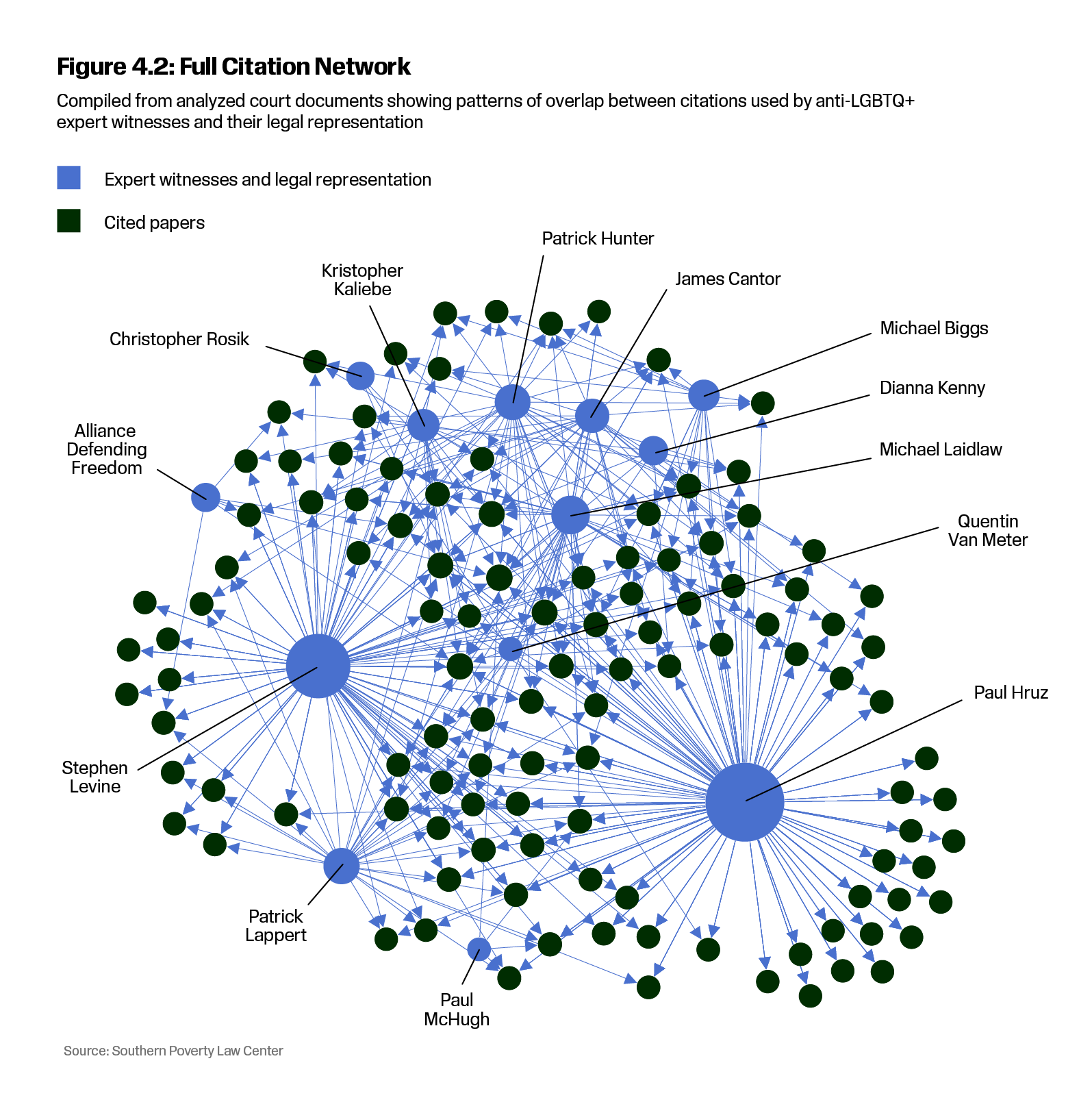
The network core comprised 54/114 publications (47.37% of total set) cited by 13/14 (92.86%) authors. The mere presence of a source in this core network should not necessarily be taken as an indication that the source is itself ideologically transphobic or even endorsed by the authors citing it — only that it was extensively referenced by these expert witnesses. While many core sources were authored by expert witnesses in the pool, others were sources that the witnesses themselves took issue with and cited in order to critique. Mere presence in the network does not convey information on how the authors engaged with a particular source — only that such engagement was present.
For instance, two papers tied for the most central spot in the network. One was, indeed, a centerpiece for anti-trans arguments in general — the original paper articulating the discredited theory of rapid-onset gender dysphoria (ROGD).[21] This paper had serious methodological, conceptual and procedural flaws that led to an extensive correction and republication (for details, see Chapter 2). Nevertheless, the paper is a staple of arguments against gender-affirming care for minors[22] because if it were true, it would suggest that the bulk of youth presenting for care: (a) are dissimilar enough from prior samples that any evidence for benefits could not be applied to them, and (b) are unlikely to be really trans, and therefore will likely regret transition should they access it. The expert witnesses thus uncritically accept Littman‘s (2018) findings as established fact, and either ignore widespread criticisms of the paper (e.g., Levine, Hruz) and/or dismiss them as authoritarian “silencing” of sound science (e.g., Levine, Hruz, and Kaliebe). Kaliebe defends the hypothesis by claiming falsely that the “re-editing” of Littman (2018) in PLOS ONE was “not a correction as claimed by activists” and that “there was no finding of error, misconduct, or faulty methods.”[23] Kaliebe made these claims despite the notice of these events on PLOS ONE being titled, “Correction: Parent reports of adolescents and young adults perceived to show signs of a rapid onset gender dysphoria,” and despite the second sentence of that paragraph stating, “The post-publication review identified issues that needed to be addressed to ensure the article meets PLOS ONE’s publication criteria.”[24] In reality, the correction was a substantial change to the original article and had to recontextualize its findings in order to avoid dramatically overstating its case.
However, the paper tied with Littman (2018) in centrality was a generally well-executed long-term retrospective, records-based study that analyzed the psychiatric hospitalizations, mortality rates (with particular attention paid to suicide and suicidality), and criminal convictions according to obtainable records for all individuals in Sweden who had successfully obtained genital surgery and changed their legal gender (which, at the time, required genital surgery) between 1978 and 2003.[25] The study–often referred to euphemistically as the Swedish Study — is thorough: It constructed two comparison/control groups from the general population using age and sex-matched controls–one matching sex to assigned sex at birth and one matching affirmed sex after legal change. However, the expert witnesses oversimplify and thereby misrepresent what this study actually found. While it does, as they claim, find ongoing health discrepancies between transgender people and these matched comparison groups over time, the authors only actually found that suicide was 19.1 times more likely and that cardiovascular disease was 2.5 times more likely among people who transitioned between 1973-1988; the discrepancies in question were much weaker for the younger cohort (1989-2003). The paper attributes these discrepancies not to the younger cohort needing greater time for them to become apparent, but to shifting social acceptance and minority stress. As dire as these discrepancies are, this highlights they may be much worse among people who desired, but could not obtain, gender-affirming surgeries.
The lead author, Dr. Cecilia Dhejne, has gone on the record to decry misuse of this reference in these ways.[26] It’s also worth noting that Dhejne does not view these discrepancies as inevitable given the cohort effects she observed. In her own words:
“The difference we observed between the 1989 to 2003 cohort and the control group is that the trans cohort group accessed more mental health care, which is appropriate given the level of ongoing discrimination the group faces. What the data tell us is that things are getting measurably better and the issues we found affecting the 1973 to 1988 cohort group likely reflects a time when trans health and psychological care was less effective and social stigma was far worse.”
As such, being central to the arguments of these expert witnesses does not mean that it’s a compromised or discredited paper. However, it does speak to another strategy used to manufacture doubt by these expert witnesses: they cherry-pick the segments of papers they find most convenient to their argument and omit any inconvenient context that contradicts the argument they want to make on the basis of the paper that they are citing. Such tactics aren’t restricted to Dhejne and colleagues (2011): a common rhetorical point among these expert declarations is arguing that if one accepts that gender-affirming care is (or may be) harmful, then these harms will disproportionately impact “vulnerable” populations. However, they do not engage with the sources they cite to make these claims beyond referencing them to indicate ostensible “overrepresentation” of gender dysphoria among these groups.
For example, Hruz and Levine solely reference Rider (2018) to argue that “children of color” are “disproportionately affected by gender discordance.”[27] Yet they neglect to clarify two key points that render their claims misleading. First, the study they cite was “unable to assess whether youth were interested in being perceived as a different gender, had received any gender-affirming medical interventions (i.e., puberty blockers and gender-affirming hormones), or had socially transitioned to their affirmed gender, which may impact how their gender expression is perceived and how they feel about particular perceptions of their gender.” Claiming the study as evidence that “experimentation” is disproportionately likely to affect students of color is, therefore, misleading. Second, the study was primarily about health care utilization by these youth within a school system, and how fear of discrimination may impede that utilization, thereby exacerbating health discrepancies, and discussing potential roles school nurses can play in assisting transgender and gender-nonconforming students. The paper even draws attention to bathroom bills forcing students to use the bathroom in the nurses’ office for safety when discussing these matters.[28]
In a similar vein, they reference both Kaltiala-Heino et al. (2015) as evidence that “gender discordance” is overrepresented among children with histories of psychiatric diagnoses, but this is actually the inverse of what that paper finds. The paper did not assess a wide pool of children with psychiatric diagnoses and find that children in that population were more likely to express cross-gender identities; it found that among children already presenting to a Finnish gender identity clinic, comorbid psychiatric diagnoses were common. No conclusions could be drawn from that paper about whether any particular child with a psychiatric diagnosis is more likely to self-identify as transgender; it merely argued that because no causal order could be established, one could not assume that transgender identity caused the overrepresentation of mental illness.
In this case, what the authors did not cite is as important as what they did cite: in 2015, Kaltiala-Heino and colleagues reported that “severe psychopathology” was common among youth presenting for care under her auspices, with depression (64%), anxiety (55%), and suicidality (53%) being the most common. However, that same team later found that need for psychiatric care due to these specific causes was significantly reduced among a sample of patients at that same clinic (depression: 54%–> 15%; anxiety: 48%–> 15%; suicidality/Self Harm: 35%–>4%) after gender-affirming hormones (Kaltiala-Heino et al., 2020). While Kaliebe does cite this study in his expert declaration, he omits these details to focus on the finding that overall need for any kind of psychiatric care for a number of other conditions (e.g., autism, ADHD) did not decrease.
It’s also broadly important to note that many of the core papers (27/54; 50%) were neither primary studies nor systematic reviews. Rather, they were commentaries, editorials, narrative reviews, or perspective pieces. While such output is an important part of the scientific record, it should nevertheless not be conflated with studies or systematic reviews, as these forms of contribution typically represent the subjective (however informed) positions of their authorship. Depending on the individual journal, such documents may not be subject to full peer review; according to emails from the Endocrine Society’s editorial board for the Journal of Clinical Endocrinology & Metabolism, they noted that “[u]sually the handling editor with [sic] make a decision on a letter to the editor without peer review, but occasionally an external reviewer will be invited. It is at the editor’s discretion.”[29] One commonly cited publication – “Growing Pains,” co-authored by expert witnesses Paul Hruz and Paul McHugh —explicitly was not, as The New Atlantis employs editorial review exclusively.[30] The relative importance of this document is in and of itself suspect, as The New Atlantis was founded by the Ethics and Public Policy Center, a conservative think tank now led by former Heritage Foundation fellow Ryan T. Anderson, which is also attached to Project 2025 as a coalition partner.
The expert witnesses themselves being authors — or at least closely associated scholars with the authors — of such documents was not uncommon. Several sources were also written by affiliates of known groups discussed elsewhere (Chapter 2 & Chapter 5): ACPeds, SEGM and its predecessor, Pediatric and Adolescent Gender Dysphoria Working Group (PAGDWG), including a number of our analyzed expert witnesses such as Michael Biggs,[31] Stephen Levine,[32] Paul Hruz,[33] Michael Laidlaw,[34] Quentin Van Meter[35] and James Cantor.[36] Notably, Biggs omitted his affiliation with SEGM entirely from his publications despite having been with them for over three years since the organization’s founding.[37]
Such omissions are not uncommon in the referenced papers: one of the most commonly cited papers, a letter to the editor called “One Size Does Not Fit All: In Support of Psychotherapy for Gender Dysphoria” included expert witness Dianna Kenny and SEGM’s president Roberto D’Angelo, yet D’Angelo didn’t disclose his role as president.[38] Further, despite Quentin Van Meter publicly (and falsely) boasting on ACPeds’ official website about the role of ACPeds authors in a letter to the editor [39] [40]
Such publications are often explicitly joint collaborations between ostensibly secular actors (SEGM) and known apparatuses of the Christian Right (ACPeds). Multiple Letters to the Editor cited are co-authored by William Malone, SEGM’s board secretary since its inception, alongside ACPeds members Michael Laidlaw, Paul Hruz and Quentin Van Meter, all of whom are frequent expert witnesses in cases involving LGBTQ+ rights.[41] Such collaboration and coordination isn’t restricted to publishing either: ACPeds membership (including Michael Laidlaw) and SEGM membership (William Malone) were both included in Deutsch’s secret working group. Their letter to the editor concerning the Endocrine Society Guidelines neither grounds their “concerns” in sound literature,[42] nor makes a convincing case about the quality of the studies, given that “hypothesis-driven randomized controlled clinical trials” are impractical bordering on impossible for puberty blockers and gender-affirming hormones.[43] [44] [45]
However, in emails exchanged within the working group, Malone and Laidlaw express a joint goal beyond editorial letters. As Figure 4.3 shows, Laidlaw claims an “ultimate, long term goal” is to “make sure that the Endocrine Society is embarrassed, publicly humiliated, and sued mercilessly.”
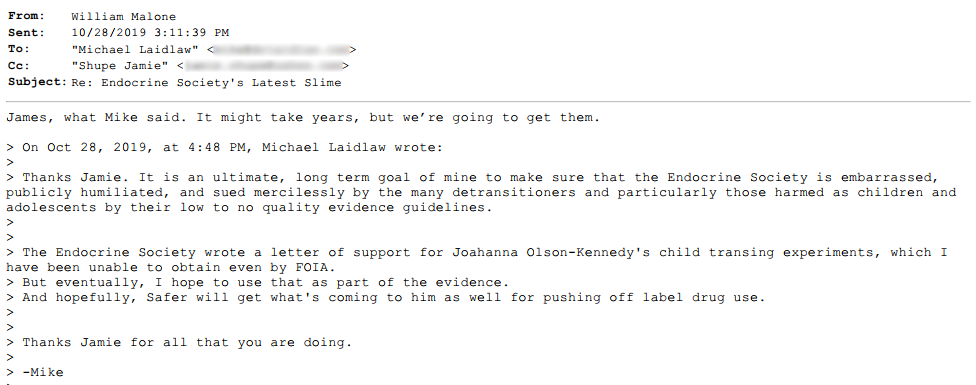
Figure 4.3: William Malone and Michael Laidlaw email with Elisa Shupe, the whistleblower of the secret working group emails covered by Mother Jones, sharing their mutual hatred of the Endocrine Society.
In the expert reports themselves, coordination appears to have occurred beyond what would be expected from chance alone. Series of citations would appear in the exact same order across multiple expert reports or declarations written by different expert witnesses between 2021 and 2023. In particular, we found heavy overlap between Stephen Levine — linked to the ostensibly secular “old guard” (see Chapter 2) through his leadership on the WPATH SOC v5, and well-connected across multiple Research & Practice groups (see Chapter 5) — and Paul Hruz of ACPeds, who has explicitly declared religious motivations.[46] Overlapping citations between Levine and Hruz are demonstrated in Figure 4.4.
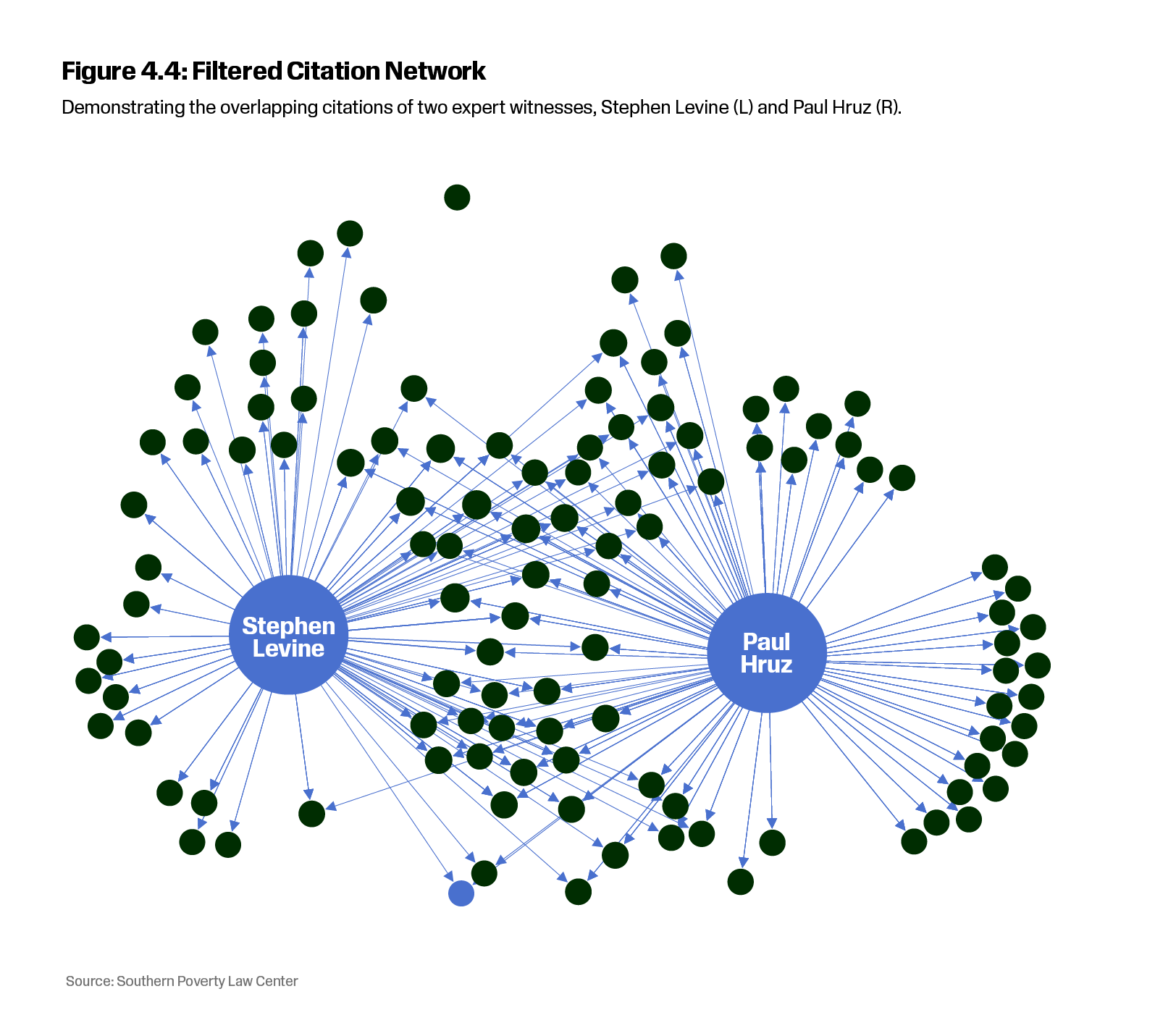
Additionally, running declarations through text comparison software revealed several word-for-word matches and other sections that were closely paraphrased between documents from Levine and Hruz, with the highest concentration in Kadel v. Folwell. In particular, the software found chunks of identical matches between the notes that Hruz submitted as part of his expert report in Kadel v. Folwell (titled “DR HRUZ’s NOTES ON RESEARCH EVALUATIONS and METHODOLOGICAL ANALYSES” [sic]) and conclusions throughout the body of Levine’s Kadel v. Folwell expert report. While this finding can’t tell us where the matching text originates from, it is alarmingly similar sounding testimony to challenge gender affirming care. Levine and Hruz are the most common expert witnesses in the cases we analyzed, and are among the most prolific expert witnesses in cases involving gender-affirming care (although both are surpassed in recent months by James Cantor).[47]
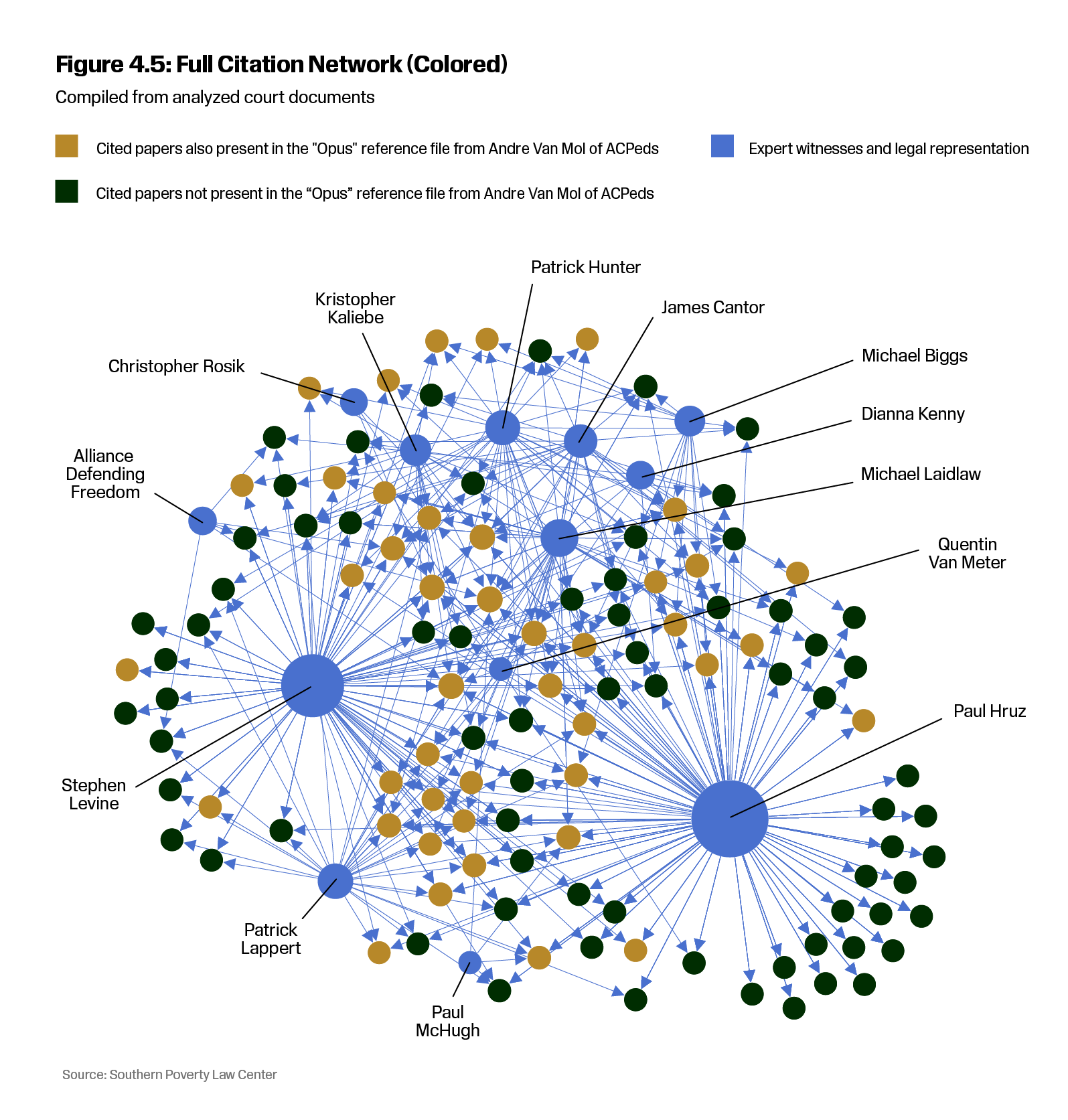
There is also significant reference overlap between expert witness contributions and the much older “Opus” file created July 14, 2019, for internal ACPeds use by Andre Van Mol. Comparing the references in this leaked file to the references in expert reports found an overlap of 43/114 (37.72%) papers overall (Figure 4.5). However, 30 of these overlapping references are in the most-cited central core, meaning that over half of the network’s core is also part of ACPeds’ internal guide for argumentation (30/54; 55.56%).
The pattern holds when analyzing just Levine and Hruz’s citations as well. Of the shared citations between the two experts, 28/51 (54.9%) were also referenced in the original Opus file (Figure 4.6).

Such overlap is striking but expected contextually. The expert witnesses themselves collaborate with one another on occasion and have multiple overlapping connections across overlapping groups (see Chapter 5). For its part, the religiously motivated ACPeds is not shy about explicitly promoting the allegedly secular SEGM. Quentin Van Meter, while giving a presentation at the God’s Voice 2022 conference held by “ex-gay” ministry First Stone Ministries, actively encouraged his eager audience to work with groups like SEGM:
“There’s a group called the Society of Evidence-Based Gender Medicine, SEGM. You should look them up because they are a reference — a beautiful scientifically based reference group that has a broad clinical spectrum of politics in terms of the backgrounds of these individuals. But what we all agree on is that the affirmation from social to medical to surgical is an abomination for these children. It is the wrong thing to do, not based on a faith base, however faith may work through you to recognize that this is what it is.”[48]
Notably, SEGM is far colder about explicitly platforming ACPeds: when the involvement of SEGM in the Deutsch secret working group came to light, SEGM’s public facing account plead ignorance, and SEGM director Julia Mason denied knowing Paul Hruz despite co-authoring papers and co-hosting symposia with him.[49]
Whether the more secular arms of these networks acknowledge it or not, their alignment in goals with the Christian Right benefits the Christian Right’s explicit goals to roll back gains for queer and trans rights (see Chapter 3). In 2017, the Values Voter Summit, hosted by Family Research Council, featured anti-trans parent activist Meg Kilgannon, who explicitly articulated the strategy to “separate the T from the alphabet soup” and to broker alliances with feminists and anti-trans liberals for this purpose (see Chapter 3).[50] Meanwhile, the ADF held meetings at their headquarters that same year in order to recruit expert witnesses for this express cause. According to deposition and trial transcripts from Brandt v. Rutledge and Dekker v. Weida, multiple anti-LGBTQ+ expert witnesses in the cases we analyzed had attended these meetings. Patrick Lappert notes meeting Paul Hruz there,[51] and Quentin Van Meter recalls attending alongside Lappert and Hruz as well as his ACPeds colleague Andre van Mol.[52] Prior to these meetings, none had ever served as expert witnesses on trans issues before, meaning that the stable of expert witnesses featured here, in this report, collected its first horses there.[53]
The Two-Pronged Strategy for Manufactured Doubt
The witnesses aim to manufacture doubt about whether youth presenting for care actually are transgender and will therefore benefit from care, while raising the possibility that their identities are actually transient phases to be outgrown or psychological delusions to be eliminated. Some (e.g., Hruz, Lappert, Van Meter) are explicitly opposed to the concepts of transgender people and gender identity in and of themselves, while others (e.g, Levine, Cantor) do not dispute that at least some youth will grow up to be transgender adults. Nevertheless, the plurality of these expert witnesses either imply, or outright state, that being transgender in adulthood should be prevented if possible given its (ostensible) risks and (ostensible) lack of benefits. These arguments are supplemented by claims that both minors and younger legal adults presenting for care are incapable of providing assent or consent for care due to either developmental stage or “vulnerabilities” (e.g., autism, depression). Some go so far as to accuse what they call the “Transgender Treatment Industry” of a nefarious conspiracy.[54]
To be clear, scientific publications that favor providing gender-affirming care to adolescents and young adults do have significant flaws and limitations, as most scientific literature does. It’s logical that arguments against providing care would focus on these shortcomings as much as possible. Thus, several core network citations were responses/criticisms to more favorable publications (14/54; 25.93%); many of them contributed to by the expert witnesses themselves, or their close associates. Of these, the majority (8/14; 57.14%) were editorials concerning one particular paper published in The American Journal of Psychiatry (Bränström & Pachankis, 2020a).
This study used the Swedish Total Population Register, a national database including all official medical diagnoses, hospitalizations, and procedures for the Swedish population over the relevant time period (2005-2015), to investigate all living individuals in the register who had not left Sweden by 2015 who had diagnoses of either transsexualism (per ICD-10) or gender-identity disorder (per DSM-IV-TR) to attempt to side-step design limitations of cohort studies. They investigated the odds of treatment for mood and/or anxiety disorders and hospitalization following a suicide attempt as a function of years since (a) initiation of hormone-suppressing treatment and (b) last gender-affirming surgery (irrespective of what that surgery was) during the year 2015. Years since hormone initiation was not associated with the likelihood of mental health treatment (operationalized as taking prescribed medication and/or outpatient health care for mood and/or anxiety disorders); years since most recent gender-affirming surgical treatment was associated with reduced likelihood of treatment for mood or anxiety disorders (but across all timepoints), these rates remained much higher compared to the general population lacking any specific diagnosis for gender incongruence. Given the small overall number of hospitalizations because of suicide attempts in 2015 (20), no conclusions could be drawn regarding suicide attempts.
On the basis of these findings, the authors initially concluded that:
“In this first total population study of transgender individuals with a gender incongruence diagnosis, the longitudinal association between gender-affirming surgery and reduced likelihood of mental health treatment lends support to the decision to provide gender-affirming surgeries to transgender individuals who seek them.”
The authors have since acknowledged that this conclusion was “too strong” given the limitations imposed by their design.[55] The restricted assessment period left anyone who either left Sweden, or died prior to 2015, unaccounted for;[56] the total population registry only encapsulated people who had a formal diagnosis, and was likely a drastic undercount of the total transgender population in Sweden.[57] Further, no reasonable comparisons could be drawn between people who obtained gender-affirming surgeries and people diagnosed with transsexualism/gender-identity disorder who had not undergone surgeries because the authors knew nothing about the health care desires or gender identities of the people whose data they analyzed.[58] While multiple letters to the editor demanded such a comparison be made, and they found no difference between the mental health of these groups, such comparisons are uninformative because those who did not undergo surgeries may not have even wanted them in the first place.[59]
Scrutiny of the paper resulted in two statistical reviewers analyzing the study itself and the letters to the editor. They did not find fault with the actual results of the paper that the authors presented, and they did find that the authors had overextended their conclusions given that no causal inferences could be drawn here.[60] This constitutes a minor correction–it does not, as Hruz asserts, constitute “recanting” their study or emphasizing that it provides “no reliable evidence” of benefit, nor does it constitute a retraction, contrary to claims made by Laidlaw,[61] Levine,[62] Lappert,[63] Cantor[64] and ACPeds’ website.[65] Further, the fact that many of the limitations raised by the letter writers were discussed in the paper itself even before the correction renders Hruz’s insinuation that the authors had “attempted to manipulate and misreport the findings of the study” quite dubious.
Similar arguments are made throughout the expert declarations regarding other papers in the literature and their associated limitations, and many of these are, in and of themselves, apt criticisms. For instance, while Turban’s work does demonstrate that among participants in the 2015 USTS survey, participants who reported both wanting and obtaining puberty blockers reported better outcomes than those who wanted, but did not obtain puberty blockers, that data remains limited owing to its nature as self-reported, snowball-sampled data, as charged by D’Angelo and colleagues (2020). It’s also true that the majority of research on gender-affirming care for transgender minors is low quality under various quality rating guidelines (Chew et al., 2018; Hembree et al., 2017).
However, limited evidence is still evidence — and sometimes, evidence is limited due to realistic, logistical constraints, such as the impracticality of conducting the RCTs necessary to establish high-quality evidence under most rating schemes.[66] Even low-quality evidence with limitations can be, and frequently is, foundational for scientific and medical practice where higher quality evidence is infeasible, impossible, or unethical to collect.[67] Further, low-quality evidence is still superior to speculation, anecdotes, and personal opinions — none of which actually constitute any evidence.
Therein lies the double standard many of these expert witnesses use to manufacture doubt: they use critical reasoning and attention to detail when they question the evidence in favor of gender-affirming care, but abandon these faculties when providing evidence against gender-affirming care, invoking severely outdated models and theories and speculative opinions as if they were established, indisputable facts.
In keeping with this broader pattern, the expert witnesses accept as factual models built on clinical, non-representative samples from the mid-20th century. Even though the “traditional profiles”of youth presenting at gender clinics were largely produced through parents bringing effeminate boys that they viewed as problematic and desired to “fix” to gender clinics to undergo what is now described as conversion therapy,[68] the authors of these expert reports still present the “sex ratio shift” to “adolescent females” seeking care as a problem that warrants solving and can only be explained through ROGD — ignoring that many of the same studies that describe this shifting ratio raise multiple plausible explanations (including shifting referral patterns)[69] for its existence that these experts do not engage with.
A central claim across these arguments is that “left to their own devices” or “without intervention,” a large percentage of youth specifically with “gender dysphoria” — up to 80-98% — will “revert” or “re-align” to identifying with their “natal” sex, which they term “desistance.” Accepting this as true, they argue that providing gender-affirming care to youth is harmful because they are not truly trans and will therefore regret care if provided, the results of which may be irreversible depending on the particulars of treatment. However, the supporting evidence for these claims is severely flawed and has come under extensive scrutiny in recent years,[70] even if these statistics were once unquestioned both in the scientific literature, in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV, DSM-IV-TR, DSM-5), the WPATH Standards of Care v7 (SOC7), and the Endocrine Society’s 2017 guidelines (Hembree et al., 2017). Checking the most common reference for these claims (Cantor, 2020) reveals several of these problems.
None of the studies Cantor reviewed used modern diagnostic criteria. Further, the most “recent” study expert witnesses point to (Singh et al., 2021) isn’t even the most recent dataset Cantor (2020) reviews, as it is the published version of a 2012 doctoral dissertation that used data collected between 1975 and 2002. The majority of these datasets (7 of 11) Cantor (2020) reviewed predate the DSM-III, much less the DSM-5, and it is unclear how many of these youth ever expressed cross-gender identification in the first place. Many were not even diagnosed with gender-identity disorder but were “subthreshold.” Additionally, many more were never diagnosed with anything because their data predated the use of diagnostic categories specific to trans people in the DSM. Moreover, the context under which these studies were conducted matters: homosexuality was still pathologized explicitly in the DSM until 1974 and was not fully removed from the DSM until 1987. Gender nonconformity in and of itself was pathologized, even outside of cross-sex identification. The simple fact is that many of these youth may never have been trans to begin with (Zucker, 2018).
Several other issues with both these earlier studies and even the more recent studies in the dataset have been raised—chief among them being that “desistance” was not explicitly operationalized as “re-identifying” with one’s birth sex in these studies given that (a) one cannot re-identify with a sex one never dis identified from in the first place and (b) for large segments of the dataset, participants were simply unavailable, and desistance was inferred rather than confirmed on the basis of supposition. All “desistance” indicated was the resolution of what was then called “gender-identity disorder” – and it is notable that many participants in these studies were never actually diagnosed as such in the first place, being as they were “sub-threshold” (and desistance was higher among subthreshold participants).
Secondly, youth in several of these studies were very explicitly not “left to their own devices.” Rather, they were explicitly subjected to psychotherapies that were, by the explicit admission from their architects, intended to make them stop engaging in gender atypical behaviors ranging from crossdressing to simply playing with counter-stereotypical toys. Kosky (1987)[71] explicitly subjected eight Australian children to inpatient conversion therapy.
Kenneth Zucker’s approach to treating children diagnosed with gender-identity disorder (GID) was explicitly to “avoid [adult transsexualism]” if at all possible, and he frequently blamed parents who insufficiently policed their child’s “cross-gendered behavior” for, in his view, increasing the likelihood of such an outcome.[72] [73] [74] [75] [76] Zucker explicitly described adult transsexuality as a negative outcome, and argued in favor of maximizing the odds of desistance and minimizing the odds of persistance — although he distinguished between treatment for prepubescent children (for whom he thought these treatments could succeed) and adolescents (for whom he believed that ”prevention of transsexualism” was no longer as feasible). [77] [78] His frequent collaborator, J. Michael Bailey, described Zucker’s rationale thusly:
“[…] Zucker believes that most boys who play with girls’ things often enough to earn a diagnosis of GID would become girls if they could. Failure to intervene increases the chances of transsexualism in adulthood, which Zucker considers a bad outcome. […] Why put boys at risk for this when they can become gay men happy to be men? I have not heard anyone argue that transsexualism is an acceptable outcome for feminine boys.”[79]
His predecessor as Archives of Sexual Behavior’s editor-in-chief, Richard Green, author of The Sissy Boy Syndrome (1987), openly stated as late as 2017 that “it is a helluva lot easier negotiating life as a gay man or lesbian woman than as a transwoman or transman,”[80] and that this therefore justified attempting to dissuade youth from seeking to transition as adults.
Cantor and Levine expressed similar opinions. Levine argued that because family dynamics may be strained by transgender transitions and because transgender people (according to his own intuitions and individual, subjective observations) have difficulties finding romantic partners, transition in and of itself constitutes a social risk. Speculation and subjective personal observations are liberally used by these expert witnesses in service of these claims—particularly observations by Levine (2017; 2019) and Zucker (2017, 2018).
However, Dr. Karl Bryant, a survivor of Green’s conversion therapy who did grow up to be a cisgender gay man, has nothing kind to say about Green’s approach and admits that his relationship with his parents never recovered. As he told the UCLA press, “Green emphasized to Bryant the advantages of being a boy and told his parents to promote masculine conduct at home.”[81] This hardly constitutes being “left alone.” Bryant has written extensively about his experiences at Green’s clinic. Further, Bryant and his contemporaries were brought to these clinics explicitly by parents who rejected their behaviors and desired to “fix” them—a desire that Levine appears sympathetic towards.
None of the expert witnesses meaningfully engage with these problems. Instead, they present the “desistance” data as straightforward facts as though none of the above were relevant. Often, they do not even directly engage with the “desistance” studies themselves at all, preferring to reference more recent subjective reflections on these studies (e.g., Cantor, 2020; Zucker, 2017; 2018). The same generous lens through which they view the early, foundational research by Kenneth Zucker and his associates at the CAMH Gender Identity Clinic (formerly the Clarke Institute) is decidedly not applied to current research that purports to support gender-affirming care.
The net effect of these double standards is that if a study’s (limited) findings might provide support for gender-affirming care, these expert witnesses often employ any and all critical faculties to discredit it; whereas if there’s even a remote chance that undesirable side effects of gender-affirming treatments might occur at some point in the future, that is treated as sufficient evidence of harm to justify banning the procedure. By that logic, one might as well ban aspirin because it can conceivably cause internal bleeding.[82] Further, on the basis of speculation, opinion and anecdotes, they uncritically argue in favor of psychotherapy aimed at preventing youth from being transgender in adulthood — despite having, by their own admission, extremely limited evidence at best for this position.
Per Levine in Kadel v. Folwell, “there is no credible, reliable-valid scientific evidence beyond anecdotal reports” that describe how psychotherapy aimed at preventing youth from being transgender could benefit them.[83] This is particularly salient as Hruz refers to “conversion therapy” as an ideologically loaded term, whereas other expert witnesses (e.g., Cantor, Levine) attempt to distinguish gay conversion therapy from efforts to change gender identity (despite their historical confluence in the studies Cantor himself reviewed). Unlike gender-affirming care, evidence of effectiveness is not required for conversion therapy.
At this point in time, judges have reviewed all these arguments, and some early patterns that emerged demonstrate what works and what doesn’t in pursuit of engendering doubt as to the necessity, efficacy, and safety of gender-affirming care.
Conclusion: What Sticks to the Wall
U.S. District Judge Robert Hinkle of Florida was particularly scathing in his assessment, quickly identifying the double standards at play. First, he highlighted Hruz and Lappert’s clear, obvious fundamental dismissal of transgender identities as a critical flaw in their ostensible “expertise” for Dekker v. Weida:
“…one of the defendants’ experts, Dr. Paul Hruz, joined an amicus brief in another proceeding asserting transgender individuals have only a “false belief” in their gender identity — that they are maintaining a “charade” or “delusion.” An AHCA consultant, Dr. Patrick Lappert — a surgeon who has never performed gender-affirming surgery — said in a radio interview that gender affirming care is a “lie,” a “moral violation,” a “huge evil” and “diabolical.” State employees or consultants suggested treatment of transgender individuals is either a “woke idea” or profiteering by the pharmaceutical industry or doctors.”[84]
In that same ruling, Hinkle pointed out the obvious problem with highlighting “low quality” of research designs in favor of transgender care while presenting no evidence that alternatives would be even remotely helpful:
“A methodology often used for evaluating medical studies — for evaluating research-generated evidence on the safety and efficacy of any given course of treatment – is known as Grading of Recommendations, Assessment, Development and Evaluation (“GRADE”). The defendants stridently assert that the evidence supporting the treatments at issue is “low” or “very low” quality as those terms are used in the GRADE system. But the evidence on the other side – the evidence purportedly showing these treatments are ineffective or unsafe – is far weaker, not just of “low” or “very low” quality. Indeed, evidence suggesting these treatments are ineffective is nonexistent.”[85]
Georgia U.S. District Judge Sarah E. Geraghty also pointed out this double standard:
“In fact, the record shows that less than 15 percent of medical treatments are supported by “high-quality evidence,” or in other words that 85 percent of evidence that guides clinical care, across all areas of medicine, would be classified as “low-quality” under the scale used by Defendant’s experts. Defendants did not refute Dr. McNamara’s testimony on this point and indeed they “concede” that “low-quality” evidence “can be considered.” In this respect, then, the fact that only “low-quality” evidence is available to support hormone therapy reveals little in itself. The Endocrine Society has produced clinical recommendations based on “low quality” or “very low quality” evidence in several areas, and such evidence supports other treatments that are uncontroversial.”[86]
Particular attention here was paid to double standards between a high threshold of evidence for benefits, but a low threshold of evidence for risks, or for efficacy of conversion therapy:
“Defendants’ experts’ insistence on a very high threshold of evidence in the context of claims about hormone therapy’s safety and benefits, and on the other hand their tolerance of a much lower threshold of evidence for claims about its risks, the likelihood of desistance and/or regret, and their notions about the ideological bias of a medical establishment that largely disagrees with them. That is cause for some concern about the wight to be assigned to their views, although the Court does not doubt that those they express are genuinely held.”[87]
In Brandt v. Rutledge, U.S. District Judge James M. Moody Jr. not only echoed these points, but went so far as to highlight the level of coordination between expert witnesses while striking down Arkansas’ gender-affirming care ban, as well as disqualifying them as experts given their religious and ideological motivations:
“Like Professor Mark Regnerus and Dr. Paul Hruz, Dr. Lappert was recruited by the Alliance Defending Freedom (“ADF”) at a seminar held in Arizona. The meeting was held to gather witnesses trained in various fields that would be willing to testify in favor of laws passed that limit transgender care. The ADF is an organization committed to protecting God’s design for marriage and family. The ADF is not a scientific organization, but a Christian-based legal advoacy group. While there is nothing nefarious about an organization recruiting witnesses to testify for their cause, it is clear from listening to the testimony that Professor Mark Regnerus, Dr. Paul Hruz, and Dr. Lappert were testifying more from a religious doctrinal standpoint than that required of experts by Daubert…
Most of the State’s expert witnesses, Professor Mark Regnerus, Dr. [Patrick] and Dr. Paul Hruz, were unqualified to offer relevant expert testimony and offered unreliable testimony. Their opinions regarding gender-affirming medical care for adolescents with gender dysphoria are grounded in ideology rather than science.”[88]
Judge Moody also highlighted the double standard at play:
“The legislative findings in Act 626 assert that there is insufficient evidence of the efficacy of gender-affirming medical care for minors. Some of the state’s expert witnesses – Dr. Levine and Dr. Hruz – offered opinions to that effect. The Court does not credit these opinions because it finds that the evidence showed that decades of clinical experience in addition to a body of scientific research demonstrate the effectiveness of these treatments. For the same reason, the Court finds that the treatments banned by Act 626 are not “experimentation” on youth, suggested by the Act’s title.”[89]
However, despite their rejection of experts like Hruz, Lappert and Regnerus as ideologues, the judges by and large gave credence to Dr. Stephen Levine, considering his testimony credible even though his actual arguments are extremely similar to Hruz’s. Again, text comparison software noted several exact matches between Levine and Hruz’s claimsrelied on the same body of antiquated evidence (e.g., “desistance” studies), speculation, opinion-based perspectives, commentaries, and letters to the editor presented as though they were factually defensible accounts, and misrepresentations of the relative evidence for benefits vs. (speculative) risks.
Why the discrepancy, if Levine and Hruz make the same arguments using the same evidence?
Demeanor, presentation and formal credentials may hold the answers. Hruz is repeatedly perceived by judges as hostile, “deeply biased,” and “inflammatory,” rather than as an expert. His disparaging on-record remarks accusing the parents of transgender youth of “abuse” for affirming them also did him no favors in court. Quentin Van Meter, Patrick Lappert and many of the other expert witnesses explicitly recruited by ADF or affiliated with ACPeds have faced similar scrutiny and dismissal.[90]
Levine, in contrast, faces no such problems. As far as credentials go, he has longstanding experience treating both transgender youth and adults (having led WPATH’s SOC5 drafting committee). Both Judge Hinkle (Florida) and Judge Moody (Arkansas) explicitly draw attention to his formal expertise as a factor distinguishing him from other witnesses they found less credible (e.g., Judge Moody: “Dr. Levine was the State’s only expert witness who has experience treating patients with gender dysphoria.”[91] And Judge Hinkle: “The elephant in the room should be noted at the outset. Gender identity is real. The record makes this clear. The medical defendants, speaking through their attorneys, have admitted it. At least one defense expert also has admitted it. That expert is Dr. Stephen B. Levine, the only defense expert who has actually treated a significant number of transgender patients.”[92]).
Further, he is more than capable of stating his case while avoiding the obvious appearance of bias and extremism. His views, even if they are rooted in the same evidence as his more extreme interlocutors (e.g., Hruz), are not dismissed as ideological because he can more plausibly claim to be advocating due caution given his experience as an expert practitioner. It must be acknowledged that when questioned, Levine will claim that he does not support unilaterally banning care for minors — despite serving as an expert witness defending a law that unilaterally bans gender-affirming care for minors, on behalf of the Alliance Defending Freedom. Even if he is compensated by, and explicitly working for, a group whose aims are not congruent with his own, he will, when pressed, describe reservations rather than make explicitly conspiratorial or hostile statements.
As such, even judges who rule against his testimony or find it unconvincing nevertheless describe Levine personally as a credible witness (e.g., Judge Hinkle: “He addressed the issues conscientiously, on the merits, rather than as a biased advocate.”[93] And Judge Moody: “The Court found Dr. Levine a very credible witness who struggles with the conflict between his scientific understanding for the need for transgender care and his faith.”[94]).
James Cantor has employed similar tactics when serving as an expert witness — although he has one key weakness that Levine lacks, as highlighted in the preliminary injunction in Eknes-Tucker:
“On cross examination, however, Dr. Cantor admitted that: (1) his patients are, on average thirty years old; (2) he had never provided care to a transgender minor under the age of sixteen; (3) he had never diagnosed a child or adolescent with gender dysphoria; (4) he had never treated a child or adolescent for gender dysphoria; (5) he had no personal experience monitoring patients receiving transitioning medications; and (6) he had no personal knowledge of the assessments or treatment methodologies used at any Alabama gender clinic. Accordingly, the Court gave his testimony regarding the treatment of gender dysphoria in minors very little weight.”[95]
Nevertheless, Cantor has not been written off so easily. In Koe v. Noggle, Cantor’s representations of systematic reviews and claims that no strong conclusions about the efficacy of care for minors could be drawn were given more weight than in Eknes-Tucker v. Ivey:
“The Court credits Dr. Cantor’s representations on matters like the content of the international systemic reviews, but the Court assigns Dr. Cantor’s views less weight as to the medical conclusions that can reasonably be drawn from evidence for the treatment of gender dysphoria in minors. As noted above, Dr. Cantor is a clinical psychologist, a sexual behavior scientist, a sex and couples’ therapist, and the Director of the Toronto Sexuality Centre. The “primary focus” of his research has been “the development of atypical sexualities” and he states that the “most impactful” of his work concerns “MRI and other biological studies of the origins of pedophilia.” He is not a physician and has no experience treating gender dysphoria in youth as such.”
In sum, the strategy that appears to work — particularly for members of the “old guard” — is to avoid the appearance of extremism by simply pointing to doubt as the reason to restrict care, while claiming that they don’t support banning care for minors per se and that they merely wish to see it heavily restricted to minimize the potential risk for harms. That these risks are inflated by these experts’ reliance on antiquated research, speculation and double standards for what constitutes firm evidence is immaterial. Even if it does not convince many federal district judges, it is plausible enough that partisan appellate court justices can, will and (increasingly) have credited it as a means to overturn injunctions and protect laws banning care against the judgments of less-partisan district judges. As explained in Chapter 5, it often falls to narrative manipulation groups to help sensationalize the doubt into moral panic against transgender people.
This potential for doubt was even highlighted in the majority opinion of the U.S. Court of Appeals for the 11th Circuit, while referencing the Dobbs precedent that overturned abortion access:
“Constitutionalizing new parental rights in the context of new medical treatments is no mean task. On the one side of the ledger, parents generally can be expected to know what is best for their children. On the other side of the ledger, state governments have an abiding interest in “preserving the welfare of children,” and “in protecting the integrity and ethics of the medical profession.” These interests give states broad power, even broad power to “limit parental freedom,” particularly in an area of new medical treatment. We doubt, for example, that there are many drug-regulatory agencies in the world that, without satisfactory long-term testing, would delegate to parents and a doctor exclusive authority to decide whether to permit a potentially irreversible new drug treatment. Judicial deference is especially appropriate where “medical and scientific uncertainty” exists. In this respect, consider the work of the Food and Drug Administration. Under a highly reticulated process that requires considerable long-range testing, the FDA determines when new drugs are safe for public use, including use by minors, and when new drugs are safe for certain purposes but not others….Gender-affirming procedures often employ FDA-approved drugs for non-approved, “off-label” uses. Tennessee decided that such off-label use in this area presents unacceptable dangers. Many medical professionals and many medical organizations may disagree. But the Constitution does not require Tennessee to view these treatments the same way as the majority of experts or to allow drugs for all uses simply becuase the FDA has approved them for some. It is well within a State’s police power to ban off-label uses of certain drugs. At the same time, it is difficult to maintain that the medical community is of one mind about the use of hormone therapy for gender dysphoria when the FDA is not prepared to put its credibility and careful testing protocols behind the use.”[96]
What allowed the U.S. Court of Appeals for the 6th Circuit to assert these claims all while stating, “we might be wrong,” in their written opinion, was credulously embracing plausible deniability–manufactured doubt. The scaremongering, hyperbolic, conspiratorial assertions Hruz, Lappert, Kaliebe, Van Meter, and other such “new guard” witnesses supplied were neither useful nor necessary, and as such, the strategies embraced by the ostensibly more “moderate” old guard (i.e., Levine, Cantor) are far more likely to be employed moving forward as litigation over gender-affirming care works its way inexorably toward a conservative Supreme Court.[97]
With 22 states having enacted restrictions on ‘transgender’ medical interventions for minors, and with courts in different states and different federal circuits reaching different conclusions in terms of upholding or overturning such laws, the battle to protect the minds and bodies of adolescent children seems ultimately destined for the Supreme Court.”
– Sarah Parshall Perry, senior legal fellow in the Edwin Meese III Center for Legal and Judicial Studies at The Heritage Foundation, responding to the ruling by the U.S. Court of Appeals for the 6th Circuit on Tennessee’s bill banning gender-affirming care for trans youth. The Daily Signal, Aug. 28, 2023.
As of Nov. 1, 2023, this scenario is no longer hypothetical: the ACLU has already asked the U.S. Supreme Court to review the 6th Circuit ruling that allowed health care bans to go into effect in Tennessee and Kentucky.[98] The Biden administration has urged the Supreme Court to hear these cases and strike down gender-affirming care bans.[99]
The core reference networks being used are consistent among the cases reviewed here and appear to be popular among other cases as well. They also appear to be more successful when used by people that aren’t easily dismissible as radicals. Erica Anderson, herself a trans woman who claims to oppose banning gender-affirming care for minors, nevertheless worked with the Alliance Defending Freedom alongside Stephen Levine in cases involving forcibly outing trans youth to their parents — successfully.[100]
Why does this work? In our opinion, the ADF sees more success with experts like Levine and Anderson because their involvement, relevant clinical expertise and claimed political positions allows the ADF to mask the extremism of the policies it is defending in court. While the ADF is infamous for its anti-LGBTQ+ and anti-abortion positions and questionable tactics like funding anti-LGBTQ+ and anti-abortion groups[101] and defending a business’s right to discriminate against hypothetical gay customers,[102] self-proclaimed moderates and liberals like Erica Anderson, Stephen Levine and James Cantor can all claim that they’re not extremists by working with the ADF, and that their individual positions are moderate and science-informed. The apparent agendas of Hruz, Lappert and Laidlaw undermine their ability to maintain such a position.
Yet, the stated positions of such experts (most notably Levine, Cantor and Anderson) are at odds with the openly stated goals and political positions of the ADF specifically and the American Christian Right in general. Unlike the European countries that these more moderate experts point towards more favorably, the American right wing will not stop at heavily gatekeeping care under the auspices of forced participation in scientific studies — they will ban it for minors, then attempt to ban it for adults, by their own admission.[103] Under the laws they are aiming to pass and defend, Anderson herself could be charged with a felony for writing letters approving select trans youth for puberty blockers and hormones. Further, if her stated position, current occupation and signature on an open letter opposing bans on gender-affirming care for minors[104] are any indication, she is not in favor of policies that ban gender-affirming care for minors — meaning her views are at odds with those of the group from which she accepts payments. Yet, Project 2025 would not discriminate between her, the youth she believes truly are transgender, and those she believes would be harmed by care. This is just like the bathroom bills ADF helped instantiate and pass don’t distinguish between her and any other trans person.[105]
While it is impossible to know their private beliefs, what matters most is that these individuals are instrumental, essential components in a far-right, religiously motivated assault on the health care rights of Americans in general, trans Americans in particular, and, left to their own devices, the rights of everyone across the world. The Christian Right, through organizations like the ADF, campaigns to reshape the world into their vision of “God’s kingdom” through their international arms. The SPLC has long studied the ADF and its campaigns, and at the time the stable of expert witnesses was being developed, concluded that “ADF’s interests are limited to having the world conform to conservative Christian principles based on those all-too-familiar ancient chronicles. Accordingly, gender affirmation is not part of God’s plan.”[106] Their funding and their activism is present globally.[107] If these experts were truly concerned about the fertility of transgender people, they might think twice before accepting money from a group that tried to defend state-mandated sterilization of transgender people across all of France.[108]
For their part, the ostensibly more “moderate” experts now have common cause with the Christian Right and with their support, groups like SEGM and Genspect are well-positioned to establish themselves as rival organizations to USPATH and WPATH in the same way that ACPeds, long ago, attempted to position itself as a rival to the AAP. They create rival think tanks,[109] rival conferences,[110] rival guidelines for “gender-exploratory therapy,”[111] and are, through their new Killarney Group, in the process of creating their own competing Standards of Care document[112] that will most likely position baseless attempts at psychoanalytic conversion therapy as the “first-line” treatment for gender dysphoria for youth under 25 years old. They even may not stop there: Genspect’s leaked discord logs reveal that its vice president would ideally have no one transition at all.[113]
Yet, the actual political and legislative power is firmly concentrated in the Christian Right’s hands. The Alliance Defending Freedom signs the checks of these experts, and solicits their input in these cases for their own ends. Therefore, our opinion is that any actual struggle of ideology between them and expert witnesses that do not wholly endorse their views would — intentionally or otherwise — help obfuscate the extremity of the policies the Christian Right champion. Regardless of what these experts personally believe in their hearts, or their immediate professional goals, the net effect of their work on behalf of the Christian Right has been to empower the cause of Christian Nationalism.
Chapter 5: Group dynamics and division of labor within the anti-LGBTQ+ pseudoscience network | Home
Resources
Endnotes
[1] An example of this is through Colin Wright, one of the advisors of the pseudoscience organization Society for Evidence-Based Gender Medicine (SEGM), responding to the retraction of a 2023 study about “rapid onset gender dysphoria” after the publisher determined the authors had failed to obtain appropriate informed consent from participants. See Wright, C. (2023, June 12). Anatomy of a Scientific Scandal. City Journal. https://www.city-journal.org/article/anatomy-of-a-scientific-scandal; See also Open Letter re: Archives of Sexual Behavior. (2023, May 5). Open Letter Re: Archives of Sexual Behavior. https://asbopenletter.com; Diaz, S., & Michael Bailey, J. (2023). Retraction Note: Rapid Onset Gender Dysphoria: Parent Reports on 1655 Possible Cases. Archives of Sexual Behavior. https://doi.org/10.1007/s10508-023-02635-1
[2] Bramoullé, Y., & Orset, C. (2018). Manufacturing doubt. Journal of Environmental Economics and Management, 90, 119–133. https://doi.org/10.1016/j.jeem.2018.04.010; Oreskes, N., & Conway, E. M. (2011). Merchants of Doubt: How a Handful of Scientists Obscured the Truth on Issues from Tobacco Smoke to Climate Change (Reprint edition). Bloomsbury Publishing.; Glantz, S. A., Slade, J., Bero, L. A., Hanauer, P., & Barnes, D. E. (Eds.). (1998). The Cigarette Papers (1st ed.). University of California Press.; Michaels, D. (2008). Doubt is Their Product: How Industry’s Assault on Science Threatens Your Health (1st edition). Oxford University Press.; Michaels, D. (2020). The Triumph of Doubt: Dark Money and the Science of Deception. Oxford University Press.; Oreskes, N. (2015). The fact of uncertainty, the uncertainty of facts and the cultural resonance of doubt. Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences, 373(2055), 20140455. https://doi.org/10.1098/rsta.2014.0455; Goldberg, R. F., & Vandenberg, L. N. (2021). The science of spin: Targeted strategies to manufacture doubt with detrimental effects on environmental and public health. Environmental Health, 20(1), 33. https://doi.org/10.1186/s12940-021-00723-0; Alumkal, A. (2017). Paranoid Science: The Christian Right’s War on Reality. NYU Press.
[3] Loris, N. (2010, October 26). How the “Scientific Consensus” on Global Warming Affects American Business—And Consumers. The Heritage Foundation. https://www.heritage.org/environment/report/how-the-scientific-consensus-global-warming-affects-american-business-and. See also Powell, J. L. (2011). The Inquisition of Climate Science. Columbia University Press.
[4] Cameron, D., & Mehrotra, D. (2023, May 2). Anti-Trans Doctor Group Leaks 10,000 Confidential Files. Wired. https://www.wired.com/story/american-college-pediatricians-google-drive-leak/
[5] American College of Pediatricians. (n.d.). Southern Poverty Law Center. Retrieved October 5, 2023, from https://www.splcenter.org/fighting-hate/extremist-files/group/american-college-pediatricians
[6] Cravens, R. G. (2023, June 5). Documents Reveal ADF Requested Anti-Trans Research From American College of Pediatricians. Southern Poverty Law Center. https://www.splcenter.org/hatewatch/2023/06/05/documents-reveal-adf-requested-anti-trans-research-american-college-pediatricians; JTEDESCO. (2014). Transgender Research Requests [PDF]. Southern Poverty Law Center. https://www.splcenter.org/wp-content/uploads/files/adf_research_requests_to_acpeds.pdf. ACPeds is also a national partner of the Promise to America’s Children, the coalition of anti-LGBTQ+ Christian Right organizations credited for drafting model bills for state legislators. See Winter, H. M. (2021, April 21). How Trans Kids Landed in the Crossfire of the Culture Wars—And the Damage It Could Do. Rolling Stone. https://www.rollingstone.com/politics/politics-features/trans-medical-bans-impact-on-trans-kids-1158853/; ABOUT US. (2021, January 30). Promise to America’s Children. https://promisetoamericaschildren.org/about-us/.
[7] Rep. Deutsch has spearheaded multiple test balloon bills targeting trans people, having also kickstarted the “bathroom bills” in 2016. While in both instances the bills were vetoed, they sparked a wave of similar anti-trans bills throughout the United States. See Diavolo, L. (2020, February 7). Trans Youth Are Being Targeted With State Laws. Teen Vogue. https://www.teenvogue.com/story/transgender-youth-targeted-state-laws-south-dakota-several-states
[8] See Chapter 5 for a detailed description of these groups and their roles in the broader ecosystem.
[9] Pauly, M. (2023, March 8). Inside the secret working group that helped push anti-trans laws across the country. Mother Jones. https://www.motherjones.com/politics/2023/03/anti-trans-transgender-health-care-ban-legislation-bill-minors-children-lgbtq/
[10] Pauly, M., & Rindlisbacher, E. (2023, May 17). A massive leak spotlights the extremism of an anti-trans medical group. Mother Jones. https://www.motherjones.com/politics/2023/05/anti-trans-american-college-pediatrics-leak-michelle-cretella-abortion/
[11] Migdon, B. (2023, June 22). Judge strikes down Florida Medicaid policy excluding gender-affirming care. The Hill. https://thehill.com/policy/healthcare/4061823-judge-strikes-down-florida-medicaid-policy-excluding-gender-affirming-care/
[12] Jones, Z. (2023, May 10). “Andre’s opinion”: Florida Medicaid agency paid thousands to a hate group leader to help ghostwrite their anti-trans policy; he copied nearly all of his sources from the hate group. Gender Analysis. https://genderanalysis.net/2023/05/andres-opinion-florida-medicaid-agency-paid-thousands-to-a-hate-group-leader-to-help-ghostwrite-their-anti-trans-policy-he-copied-nearly-all-of-his-sources-from-the-hate-g/
[13] American College of Pediatricians. (n.d.). General Resources. Biological Integrity. Retrieved October 15, 2023, from https://biologicalintegrity.org/general-resources/. See also American College of Pediatricians. (2023). Top Studies on the Science Against Transgender Interventions [PDF]. Biological Integrity. https://biologicalintegrity.org/wp-content/uploads/2023/09/Top-Studies-Fact-Sheet.pdf
[14] American College of Pediatricians. (n.d.). For Policymakers. Biological Integrity. Retrieved October 15, 2023, from https://biologicalintegrity.org/for-policymakers/
[15] Redden, M. (2023, September 15). These Paid “Experts” Are Crisscrossing The Country To Defend Anti-Trans Laws. Huffington Post. https://www.huffpost.com/entry/paid-experts-defending-anti-trans-law_n_65021a7ee4b01df7c3b6d513; Hart, D. C. (2017, December 13). Alliance Defending Freedom developed a stable of anti-LGBT “expert” witnesses. Southern Poverty Law Center. https://www.splcenter.org/hatewatch/2017/12/13/alliance-defending-freedom-developed-stable-anti-lgbt-expert-witnesses
[16] The name of the case changed due to plaintiff Rev. Paul Eknes-Tucker not being part of the appeal process. Through the course of this chapter, we refer to Boe v. Marshall as Eknes-Tucker v. Ivey, as that was the name of the case when the analyzed expert declarations and reports were filed.
[17] GLAD. (2023, August 22). Statement on 11th Circuit Ruling Reversing Injunction on Alabama Transgender Healthcare Ban. https://www.glad.org/statement-on-11th-circuit-ruling-reversing-injunction-on-alabama-transgender-healthcare-ban/
[18] Eknes-Tucker v. Governor, of the State of Ala., No. 22-11707 (11th Cir. Aug. 21, 2023), via https://casetext.com/case/eknes-tucker-v-governor-of-the-state-of-ala. See also Riess, R., Jordan, J., & Sottile, Z. (2023, July 8). Federal appeals court allows Tennessee ban on gender-affirming care for transgender minors to take effect. CNN, https://www.cnn.com/2023/07/08/politics/tennessee-gender-affirming-care-ban/index.html; L. W. v. Skrmetti, 73 F.4th 408 (6th Cir. 2023), via https://casetext.com/case/l-w-v-skrmetti-2; Dobbs v. Jackson Women’s Health Organization, 142 S. Ct. 2228, 213 L. Ed. 2d 545 (2022), via https://casetext.com/case/dobbs-v-jackson-womens-health-organization. Notably, Alliance Defending Freedom has publicized its role drafting the legislation that led to the overturning of Roe. See Kirkpatrick, D. D. (2023, October 2). The Next Targets for the Group That Overturned Roe. The New Yorker. https://www.newyorker.com/magazine/2023/10/09/alliance-defending-freedoms-legal-crusade.
[19] We counted 611 possible publications to review and annotate according to rubrics we designed. For feasibility, we exclusively reviewed sources that were (a) published in an academic or scientific journal and (b) were cited in the majority (3/4) of cases that we analyzed, yielding a list of 123 publications as candidates for full review. Full books (e.g.,The Sissy Boy Syndrome by Richard Green) or extensive standards of care that were not review papers (e.g., WPATH’s Standards of Care) were not reviewed according to our rubrics. Our final sample of sources to fully review encompassed 114 documents (see Appendix 4.2 for exclusion criteria and Appendix 4.3 for the full list of 123 candidate publications). Excluded documents were still reviewed–but were not scored or used in subsequent citation-based analyses.
[20] Two documents, one from Joseph Zanga and one from Sophie Scott, had to be excluded from connection analysis due to either not citing their claims or not providing a reference page to verify the citations included (respectively).
[21] Littman, L. (2018). Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLOS ONE, 13(8), e0202330. https://doi.org/10.1371/journal.pone.0202330. See also Ashley, F. (2020). A critical commentary on ‘rapid-onset gender dysphoria.’ The Sociological Review, 68(4), 779–799. https://doi.org/10.1177/0038026120934693. An example of this claim can be found in Kadel v. Folwell, Doc. 215-3, Hruz Decl. ¶ 66.
[22] Kesslen, B. (2022, August 18). How the idea of a “transgender contagion” went viral—And caused untold harm. MIT Technology Review. https://www.technologyreview.com/2022/08/18/1057135/transgender-contagion-gender-dysphoria/; Sun, S. D. & Ashley, F. (2023, November 6). Anti-Trans Myths. https://www.openmindmag.org/articles/anti-trans-myths?fbclid=IwAR3QtmdF3HAiCsovpEgG3kpcUvQZwZ-Sgvn50o8jKhQjWmtm0ld_7Dzel0o; McLamore, Q. (2023, January 23). Disarming transphobia. https://aeon.co/essays/the-real-reason-why-theres-a-global-rise-in-trans-youth
[23] Dekker v. Weida, 4:22-cv-00325-RH-MAF, Kaliebe Report ¶ 87.
[24] Littman, L. (2019). Correction: Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLOS ONE, 14(3), e0214157. https://doi.org/10.1371/journal.pone.0214157
[25] Dhejne, C., Lichtenstein, P., Boman, M., Johansson, A. L. V., Långström, N., & Landén, M. (2011). Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden. PLOS ONE, 6(2), e16885. https://doi.org/10.1371/journal.pone.0016885. See also Williams, C. (2015, November 2). Fact check: Study shows transition makes trans people suicidal. TransAdvocate. https://www.transadvocate.com/fact-check-study-shows-transition-makes-trans-people-suicidal_n_15483.htm. An example of this claim can be found in Kadel v. Folwell, Doc. 215-1, Levine Decl. ¶ 74.
[26] Williams (2015).
[27] Hruz and Levine make this claim in all three of their declarations, albeit at different points per document. See Kadel v. Folwell, Doc. 215-1, Levine Decl. § C ¶ 21 and Doc. 215-3, Hruz Decl. ¶ 75; Eknes-Tucker v. Ivey, Doc. 69-5, Hruz Decl. ¶ 77; Dekker v. Weida, Levine Report § C ¶ 33 and Hruz Report ¶ 138; Tingley v. Ferguson, Doc. 2-3, Levine Decl. § C ¶ 24.
[28] Rider, G. N., McMorris, B. J., Gower, A. L., Coleman, E., & Eisenberg, M. E. (2018). Health and Care Utilization of Transgender and Gender Nonconforming Youth: A Population-Based Study. Pediatrics, 141(3), e20171683. https://doi.org/10.1542/peds.2017-1683, referencing Porta, C. M., Gower, A. L., Mehus, C. J., Yu, X., Saewyc, E. M., & Eisenberg, M. E. (2017). “Kicked out”: LGBTQ youths’ bathroom experiences and preferences. Journal of Adolescence, 56, 107–112. https://doi.org/10.1016/j.adolescence.2017.02.005
[29] Dekker v. Weida, 4:22-cv-00325, (N.D. Fla.), Doc. 136-6, via https://storage.courtlistener.com/recap/gov.uscourts.flnd.443916/gov.uscourts.flnd.443916.136.16.pdf
[30] Paul Hruz, one of the authors, stated that the publication “was editorially reviewed, not sent out to people outside of the editorial board” while being cross-examined during Dekker v. Weida. See Dekker v. Weida, 4:22-cv-00325-RH-MAF, Trial Tr. 5.17.2023 901:12-902:3, inquiring about Hruz, P. W., Mayer, L. S., & McHugh, P. R. (2017). Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria. The New Atlantis. https://www.thenewatlantis.com/publications/growing-pains
[31] Biggs, M. (2022). Suicide by Clinic-Referred Transgender Adolescents in the United Kingdom. Archives of Sexual Behavior, 51(2), 685–690. https://doi.org/10.1007/s10508-022-02287-7; Biggs, M. (2020). Puberty Blockers and Suicidality in Adolescents Suffering from Gender Dysphoria. Archives of Sexual Behavior, 49(7), 2227–2229. https://doi.org/10.1007/s10508-020-01743-6
[32] Levine, S. B. (2016). Reflections on the Legal Battles Over Prisoners with Gender Dysphoria. Journal of the American Academy of Psychiatry and the Law Online, 44(2), 236–245.; Levine, S. B. (2018). Ethical Concerns About Emerging Treatment Paradigms for Gender Dysphoria. Journal of Sex & Marital Therapy, 44(1), 29–44. https://doi.org/10.1080/0092623X.2017.1309482; Levine, S. B. (2019). Informed Consent for Transgendered Patients. Journal of Sex & Marital Therapy, 45(3), 218–229. https://doi.org/10.1080/0092623X.2018.1518885; Levine, S. B., Abbruzzese, E., & Mason, J. W. (2022). Reconsidering Informed Consent for Trans-Identified Children, Adolescents, and Young Adults. Journal of Sex & Marital Therapy, 48(7), 706–727. https://doi.org/10.1080/0092623X.2022.2046221. See also Abbruzzese, E., Levine, S. B., & Mason, J. W. (2023). The Myth of “Reliable Research” in Pediatric Gender Medicine: A critical evaluation of the Dutch Studies—and research that has followed. Journal of Sex & Marital Therapy, 0(0), 1–27. https://doi.org/10.1080/0092623X.2022.2150346
[33] Hruz, P. W., Mayer, L. S., & McHugh, P. R. (2017). Growing Pains: Problems with Puberty Suppression in Treating Gender Dysphoria. The New Atlantis. https://www.thenewatlantis.com/publications/growing-pains; Hruz, P. W. (2020). Deficiencies in Scientific Evidence for Medical Management of Gender Dysphoria. The Linacre Quarterly, 87(1), 34–42. https://doi.org/10.1177/0024363919873762; Laidlaw, M. K., Van Meter, Q. L., Hruz, P. W., Van Mol, A., & Malone, W. J. (2019). Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology & Metabolism, 104(3), 686–687. https://doi.org/10.1210/jc.2018-01925; Malone, W. J., Hruz, P. W., Mason, J. W., & Beck, S. (2021). Letter to the Editor from William J. Malone et al: “Proper Care of Transgender and Gender-diverse Persons in the Setting of Proposed Discrimination: A Policy Perspective.” The Journal of Clinical Endocrinology & Metabolism, 106(8), e3287–e3288. https://doi.org/10.1210/clinem/dgab205
[34] Laidlaw et al. (2019); Van Mol, A., Laidlaw, M. K., Grossman, M., & McHugh, P. R. (2020). Gender-Affirmation Surgery Conclusion Lacks Evidence. American Journal of Psychiatry, 177(8), 765–766. https://doi.org/10.1176/appi.ajp.2020.19111130
[35] Laidlaw et al. (2019)
[36] Cantor, J. M. (2020). Transgender and Gender Diverse Children and Adolescents: Fact-Checking of AAP Policy. Journal of Sex & Marital Therapy, 46(4), 307–313. https://doi.org/10.1080/0092623X.2019.1698481
[37] SEGM no longer lists advisors on their About Us page as of writing. However, Internet archive records show Biggs as one of their advisors dating from at least July 2020 to as recently as August 3rd 2023. See https://archive.ph/yBkfy and https://web.archive.org/web/20230806155143/https://segm.org/about_us
[38] D’Angelo, R., Syrulnik, E., Ayad, S., Marchiano, L., Kenny, D. T., & Clarke, P. (2021). One Size Does Not Fit All: In Support of Psychotherapy for Gender Dysphoria. Archives of Sexual Behavior, 50(1), 7–16. https://doi.org/10.1007/s10508-020-01844-2; SEGM’s 2020 and 2021 990s filed with the United States Internal Revenue Service list D‘Angelo as their President in Part VII.
[39] Van Meter, Q. (n.d.). American Journal of Psychiatry Retracts Study: No Evidence Hormones or Surgery Help Gender Incongruent Patients. American College of Pediatricians. Retrieved October 15, 2023, from https://acpeds.org/press/american-journal-of-psychiatry-retracts-study
[40] Van Mol et al. (2020)
[41] Laidlaw et al. (2019); Malone et al. (2021). SEGM’s 2020 and 2021 990s filed with the United States Internal Revenue Service list Malone as their Secretary in Part VII.
[42] Briefly: they misrepresent Dhejne et al. (2011) similar to others described above, reference Littman (2018) as if it were unassailable fact, and misrepresent an antiquated care model used by Zucker et al. (2012) to argue that there’s ironclad proof psychotherapy can “alleviate” gender dysphoria; see Zucker, K. J., Wood, H., Singh, D., & Bradley, S. J. (2012). A developmental, biopsychosocial model for the treatment of children with gender identity disorder. Journal of Homosexuality, 59(3), 369–397. https://doi.org/10.1080/00918369.2012.653309, while also citing a review of antiquated studies that did not use modern criteria to argue that most youth “outgrow this condition,” none of which used modern diagnostic standards; see Ristori, J., & Steensma, T. D. (2016). Gender dysphoria in childhood. International Review of Psychiatry, 28(1), 13–20. https://doi.org/10.3109/09540261.2015.1115754
[43] See Howick, J., Koletsi, D., Ioannidis, J. P. A., Madigan, C., Pandis, N., Loef, M., Walach, H., Sauer, S., Kleijnen, J., Seehra, J., Johnson, T., & Schmidt, S. (2022). Most healthcare interventions tested in Cochrane Reviews are not effective according to high quality evidence: A systematic review and meta-analysis. Journal of Clinical Epidemiology, 148, 160–169. https://doi.org/10.1016/j.jclinepi.2022.04.017; Fleming, P. S., Koletsi, D., Ioannidis, J. P., & Pandis, N. (2016). High quality of the evidence for medical and other health-related interventions was uncommon in Cochrane systematic reviews. Journal of clinical epidemiology, 78, 34–42. https://doi.org/10.1016/j.jclinepi.2016.03.012; Ashley, F., Tordoff, D. M., Olson-Kennedy, J., & Restar, A. J. (2023). Randomized-controlled trials are methodologically inappropriate in adolescent transgender healthcare. International Journal of Transgender Health, 0(0), 1–12. https://doi.org/10.1080/26895269.2023.2218357
[44] Laidlaw et al. (2019)
[45] For its part, the Endocrine Society has long-since responded to Laidlaw and colleagues’ letter and criticized its oversights. See Rosenthal, S. M., Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2019). Response to Letter to the Editor: “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology & Metabolism, 104(11), 5102–5103. https://doi.org/10.1210/jc.2019-00930
[46] During the bench trial for Dekker v. Weida, Kim Hutton–a parent of a trans son from Missouri–testified that Hruz emphasized the “moral and spiritual needs of the children” and that gender affirming care was against “God’s plan” via email. See Dekker v. Weida, 4:22-cv-00325-RH-MAF, Trial Tr. 5.17.2023 768:12-772:8. Similar themes are present in his presentations for ex-gay networks such as Restored Hope Network, where he refers to how “there are many people that buy into lies about who they are as a child of God” who need reparative therapy to be made whole. See Restored Hope Network (Director). (2023, January 10). HOPE 2022—Proclaiming Truth About Sex & Gender with Charity & Love-Dr Paul Hruz MD, PhD., Keynote. https://www.youtube.com/watch?v=bfTyRCdIvks, 46:01
[47] Redden (2023).
[48] God’s Voice (Director). (2022, June 6). 2022 God’s Voice 7th Presentation "The Growing Deception of Transgender Medicine” by Dr.Van Meter. 53:23-54:00. https://www.youtube.com/watch?v=1uu3xSQTeEs
[49] Mason and Hruz appeared back-to-back at Genspect‘s Trans: A Closer Look college symposium on April 8, 2022. See Genspect (Director). (2022, June 2). Symposium 1.3 Dr. Julia Mason. https://www.youtube.com/watch?v=IWRlgrsaAlA; Genspect (Director). (2022, June 2). Symposium 1.4 Dr. Paul Hruz. https://www.youtube.com/watch?v=AZsFakJErE8. Later, Mason tweeted that SEGM would not work with members of ACPeds and that Hruz had abandoned his membership to work with them (see https://archive.ph/ovGpC). However, according to membership records between 2020 and 2022 within the leaked ACPeds Google Drive, Paul Hruz was consistently listed as an active “specialty fellow”, overlapping with when he had co-authored with Mason and fellow SEGM founder William Malone.
[50] Barthélemy, H. (2017, October 23). Christian Right tips to fight transgender rights: Separate the T from the LGB. Southern Poverty Law Center. https://www.splcenter.org/hatewatch/2017/10/23/christian-right-tips-fight-transgender-rights-separate-t-lgb
[51] Brandt v. Rutledge, 4:21-CV-00450-JM, Lappert Tr. 77:4-79:13 via https://transgender.agency/files/deposition-patrick-w-lappert-brandt-v-rutledge-2022-05-06.pdf
[52] Dekker v. Weida, 4:22-cv-00325-RH-MAF, Doc. 144-3, Van Meter Tr. 169:18-171:4, via https://transgender.agency/files/dekker-v-weida/144-3.pdf
[53] Hart, D. C. (2017, December 13). Alliance defendign freedom developed a stable of anti-LGBT ”expert” witnesses. Southern Poverty Law Center. https://www.splcenter.org/hatewatch/2017/12/13/alliance-defending-freedom-developed-stable-anti-lgbt-expert-witnesses
[54] Examples of this are predominantly in Kadel v. Folwell, where anti-trans expert witnesses argue that the so-called “Transgender Treatment Industry” has been manipulating science to push gender affirming care for profit. See Lappert Decl. § 12 ¶ 9-15, McHugh Decl. § 9-10, Hruz Decl. § 65 ¶ 1 and § 71 ¶ 6, and Levine Decl. § II. B ¶ 15 and § IV ¶ 65. Hruz also uses the term in Eknes-Tucker v. Ivey (Hruz Decl. ¶ 69) when referencing Ryan T. Anderson’s book When Harry Became Sally: Responding to the Transgender Moment. Lappert, meanwhile, also occasionally uses the term “Gender Transition Industry” (Kadel v. Folwell, Lappert Decl. Decl. § 19 ¶ 14).
[55] Bränström, R., & Pachankis, J. E. (2020b). Toward Rigorous Methodologies for Strengthening Causal Inference in the Association Between Gender-Affirming Care and Transgender Individuals’ Mental Health: Response to Letters. American Journal of Psychiatry, 177(8), 769–772. https://doi.org/10.1176/appi.ajp.2020.20050599
[56] Bränström & Pachankis (2020b); Anckarsäter, H., & Gillberg, C. (2020). Methodological Shortcomings Undercut Statement in Support of Gender-Affirming Surgery. American Journal of Psychiatry, 177(8), 764–765. https://doi.org/10.1176/appi.ajp.2020.19111117
[57] Bränström & Pachankis (2020b); Van Mol et al. (2020)
[58] Bränström & Pachankis (2020b); Wold, A. (2020). Gender-Corrective Surgery Promoting Mental Health in Persons With Gender Dysphoria Not Supported by Data Presented in Article. American Journal of Psychiatry, 177(8), 768–768. https://doi.org/10.1176/appi.ajp.2020.19111170
[59] By the authors’ own admission, for all they knew, participants who did not obtain gender-affirming surgeries didn’t want them–after all, not all people who self-describe as transgender or non-binary actually want gender-affirming surgical interventions, and by 2015, they didn’t even strictly need them to change their legal sex anymore in Sweden.
[60] Kalin, N. H. (2020). Reassessing Mental Health Treatment Utilization Reduction in Transgender Individuals After Gender-Affirming Surgeries: A Comment by the Editor on the Process. American Journal of Psychiatry, 177(8), 764–764. https://doi.org/10.1176/appi.ajp.2020.20060803
[61] Eknes-Tucker v. Ivey, Doc. 69-3, Laidlaw Decl. § I ¶ 2.
[62] Tingley v. Ferguson, Doc. 2-3, Levine Decl. ¶ 116-119.
[63] Kadel v. Folwell, Doc. 215-4, Lappert Decl. § 12 ¶ 6-7.
[64] Eknes-Tucker v. Ivey, Doc. 69-2, Cantor Decl. ¶ 52.
[65] Van Meter (n.d.), https://acpeds.org/press/american-journal-of-psychiatry-retracts-study
[66] While the attempted Cochrane review by Haupt and colleagues (2020) does call for randomized control trials to investigate the effects of antiandrogens and estrogens on feminization and their associated health risks, their main goal was to investigate which types of feminization treatment were safest, not to determine whether it was practical or ethical to provide care at all, which was not in question for that review.
[67] Koe v. Noggle, Doc. 70-1, McNamara Decl. ¶ 23–28, via https://storage.courtlistener.com/recap/gov.uscourts.gand.317779/gov.uscourts.gand.317779.70.1.pdf
[68] See Meadows, T. Trans Kids; see also: Ashley F. (2019). Shifts in Assigned Sex Ratios at Gender Identity Clinics Likely Reflect Changes in Referral Patterns. The journal of sexual medicine, 16(6), 948–949. https://doi.org/10.1016/j.jsxm.2019.03.407
[69] For example, see de Graaf, N. M., Carmichael, P., Steensma, T. D., & Zucker, K. J. (2018). Evidence for a Change in the Sex Ratio of Children Referred for Gender Dysphoria: Data From the Gender Identity Development Service in London (2000-2017). The journal of sexual medicine, 15(10), 1381–1383. https://doi.org/10.1016/j.jsxm.2018.08.002
[70] Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., Sinnott, M.-L., Jamieson, A., & Pickett, S. (2018). A critical commentary on follow-up studies and “desistance” theories about transgender and gender-nonconforming children. International Journal of Transgenderism, 19(2), 212–224. https://doi.org/10.1080/15532739.2018.1456390; Karrington B. (2022). Defining Desistance: Exploring Desistance in Transgender and Gender Expansive Youth Through Systematic Literature Review. Transgender health, 7(3), 189–212. https://doi.org/10.1089/trgh.2020.0129
[71] Kosky, R. J. (1987). Gender-disordered children: Does inpatient treatment help? Medical Journal of Australia, 146(11), 565–569. https://doi.org/10.5694/j.1326-5377.1987.tb120415.x
[72] Bradley, S. J., & Zucker, K. J. (1997). Gender identity disorder: A review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry, 36(7), 872–880. https://doi.org/10.1097/00004583-199707000-00008
[73] Morton, G. (2001, January 10). Drop the doll! Xtra Magazine. https://xtramagazine.com/health/drop-the-doll-46535
[74] National Association for Research & Therapy of Homosexuality (NARTH) explicitly championed Zucker’s approach to treatment and applied its logic to support the ostensible ethics of conversion therapy, although Zucker himself never took a firm stance in favor of anti-gay conversion therapy. See NARTH Scientific Advisory Committee. (2007). Gender Identity Disorders In Childhood And Adolescence: A Critical Inquiry And Review Of The Kenneth Zucker Research [PDF]. National Association for Research & Therapy of Homosexuality. https://web.archive.org/web/20080723195034/http:/www.narth.com/docs/GIDReviewKenZucker.pdf
[75] Spiegel, A. (2008, May 7). Two Families Grapple with Sons’ Gender Identity. NPR. https://www.npr.org/2008/05/07/90247842/two-families-grapple-with-sons-gender-preferences
[76] Zucker, K. J. (2006). Commentary on Langer and Martin's (2004) "How dresses can make you mentally ill: Examining gender identity disorder in children." Child & Adolescent Social Work Journal, 23(5-6), 533–555. https://doi.org/10.1007/s10560-006-0074-5
[77] Zucker, K. J., & Bradley, S. J. (1995). Gender identity disorder and psychosexual problems in children and adolescents. Guilford Press.
[78] Zucker, K. J., Wood, H., Singh, D., & Bradley, S. J. (2012). A developmental, biopsychosocial model for the treatment of children with gender identity disorder. Journal of homosexuality, 59(3), 369–397. https://doi.org/10.1080/00918369.2012.653309
[79] Bailey, J.. (2003). The Man Who Would Be Queen. Pp.31-32.
[80] Green, R. (2017). To Transition or Not to Transition? That Is the Question. Current Sexual Health Reports, 9(2), 79–83. https://doi.org/10.1007/s11930-017-0106-5
[81] Goulding, S. C. (2019, November 18). UCLA study tried to change children’s gender identity starting in the 1960s, say two educators. Orange County Register. https://www.ocregister.com/2019/11/18/2-subjects-discuss-trauma-as-kids-involved-in-uclas-now-defunct-gender-identity-study/
[82] See Drescher, J. (2023). Informed Consent or Scare Tactics? A Response to Levine et al.’s “Reconsidering Informed Consent for Trans-Identified Children, Adolescents, and Young Adults.” Journal of Sex & Marital Therapy, 49(1), 99–107. https://doi.org/10.1080/0092623X.2022.2080780
[83] Kadel v Folwell, Doc. 215-1, Levine Decl. ¶ 35. Stella O’Malley, the director of Genspect (which Levine is an advisor of), has similarly cautioned Genspect members that “we need to be careful in declaring we’re the ‘evidence-based side,’ as most parents seek psychotherapy for their gender distressed kids and psychotherapy doesn’t have a strong evidence base.” See Piper, E. (2023, July 25). EXCLUSIVE: “Focus relentlessly on under 25”: Leaked chats reveal influential gender-critical group’s plan to use children to push for bans on transitioning. The Daily Dot. https://www.dailydot.com/debug/genspect/. Genspect plays a major role in the application of anti-trans publications into therapeutic practice. Their role is described more in Chapter 5, Research & Practice Groups.
[84] Dekker v. Weida, 4:22cv325-RH-MAF (N.D. Fla. Jun. 21, 2023), via https://casetext.com/case/dekker-v-weida-1
[85] Ibid.
[86] Koe v. Noggle, 1:23-CV-2904-SEG, (N.D. Ga. Aug. 20, 2023), via https://caselaw.findlaw.com/court/us-dis-crt-n-d-geo-atl-div/114917398.html
[87] Ibid.
[88] Brandt v. Rutledge, 4:21CV00450 JM (E.D. Ark. Jun. 20, 2023), via https://casetext.com/case/brandt-v-rutledge-9
[89] Ibid.
[90] In Kadel v. Folwell, both Patrick Lappert and Paul McHugh had their expert testimony restricted by the court. In terms of Lappert, the court placed particular emphasis on how “references to a Transgender or Gender Treatment Industry and related conspiratorial accusations are nothing more than rank speculation designed to distract or inflame the jury and has no business in expert testimony.“ See Kadel v. Folwell, 1:19CV272 (M.D.N.C. Jun. 10, 2022), via https://casetext.com/case/kadel-v-folwell-3. Similarly, Quentin Van Meter was struck from the record as an expert witness in a divorce case where the parents were split on whether to continue gender affirming care for their trans kid. An attorney on the case noted that the courts viewed Van Meter’s testimony as agenda driven, not based in science. See Caruso, S., September 15, P. C.-S., & 2020. (2020, September 15). A Texas judge ruled this doctor was not an expert. A Pennsylvania Republican invited him to testify on trans health care. Pennsylvania Capital-Star.https://www.penncapital-star.com/government-politics/a-texas-judge-ruled-this-doctor-was-not-an-expert-a-pennsylvania-republican-invited-him-to-testify-on-trans-health-care/ https://www.penncapital-star.com/government-politics/a-texas-judge-ruled-this-doctor-was-not-an-expert-a-pennsylvania-republican-invited-him-to-testify-on-trans-health-care/
[91] Brandt v. Rutledge, 4:21CV00450 JM (E.D. Ark. Jun. 20, 2023), ¶ 291
[92] Dekker v. Weida, 4:22cv325-RH-MAF (N.D. Fla. Jun. 21, 2023), § II ¶ 3.
[93] Ibid.
[94] Brandt v. Rutledge, 4:21CV00450 JM (E.D. Ark. Jun. 20, 2023), ¶ 293
[95] Eknes-Tucker v. Marshall, 603 F. Supp. 3d 1131 (M.D. Ala. 2022), via https://casetext.com/case/eknes-tucker-v-marshall
[96] L. W. v. Skrmetti, 73 F.4th 408 (6th Cir. 2023)
[97] Totenberg, N. (2022, July 5). The Supreme Court is the most conservative in 90 years. NPR. https://www.npr.org/2022/07/05/1109444617/the-supreme-court-conservative
[98] Strangio, C. (2023, November 1). Why We’re Taking the Fight for Trans Youth Health Care to the Supreme Court. American Civil Liberties Union. https://www.aclu.org/news/lgbtq-rights/why-were-taking-the-fight-for-trans-youth-health-care-to-the-supreme-court
[99] Petittion for a Writ of Certiorari. United States of America v. Jonathan Thomas Skrmetti, et al. https://www.supremecourt.gov/DocketPDF/23/23-477/288875/20231106135238432_U.S.%20v.%20Skrmetti%20-%20Pet.pdf. Accessed 11/16/2023.
[100] See Wedward, A. (2023, October 3). WILL & ADF Secure Groundbreaking Legal Victory in Parental Rights Case. Wisconsin Institute for Law & Liberty. https://will-law.org/will-adf-secure-groundbreaking-legal-victory-in-parental-rights-case/
[101] Gabbatt, A. (2023, June 30). Revealed: Christian legal non-profit funds US anti-LGBTQ and anti-abortion organizations. The Guardian. https://www.theguardian.com/world/2023/jun/30/christian-hate-group-funding-us-anti-lgbtq-anti-abortion-organizations
[102] Grant, M. G. (2023, June 29). The Mysterious Case of the Fake Gay Marriage Website, the Real Straight Man, and the Supreme Court. The New Republic. https://newrepublic.com/article/173987/mysterious-case-fake-gay-marriage-website-real-straight-man-supreme-court. See also Grant, M. G. (2023, July 6). The Straight Man in the Gay Wedding Website Case Is Not the Real Problem. The New Republic. https://newrepublic.com/article/174113/straight-man-gay-wedding-website-case-not-real-problem.
[103] Multiple bills sought to ban gender affirming care for adults over 18, including at least two placing their upper limits at age 26. See Cole, D. (2023, February 11). GOP lawmakers escalate fight against gender-affirming care with bills seeking to expand the scope of bans. CNN. https://www.cnn.com/2023/02/11/politics/gender-affirming-care-bans-transgender-rights/index.html. Two laws restricted gender affirming care access for adults without age qualifiers. See Rosenbaum, J. (2023, April 24). Missouri to restrict gender-affirming care for trans adults this week. NPR. https://www.npr.org/2023/04/24/1171293057/missouri-attorney-general-transgender-adults-gender-affirming-health-care, Beaty, T., Farrington, B., & Schoenbaum, H. (2023, June 4). Transgender adults in Florida are blindsided that a new law also limits their access to health care. AP News. https://apnews.com/article/florida-transgender-health-care-adults-e7ae55eec634923e6593a4c0685969b2
[104] United States Professional Association for Transgender Health & World Professional Association for Transgender Health. (2021). Joint Letter from USPATH and WPATH [PDF]. WPATH. https://www.wpath.org/media/cms/Documents/Public%20Policies/2021/Joint%20WPATH%20USPATH%20Letter%20Dated%20Oct%2012%202021.pdf; Erica E. Anderson, Dianne Berg, Marci Bowers, Diane Chen, Aaron Devor, AJ Eckert, Laura Edwards-Leeper, Diane Ehrensaft, Robert Garofalo, Lisa Griffin, Alex Iantaffi, David Inwards-Breland, Laura Kuper, Scott Leibowitz, Arlene Lev, Ximena Lopez, Kristina R. Olson, Johanna Olson-Kennedy, G. Nic Rider, … Melina Wald. (2023, March 27). Statement Regarding Laws Restricting Gender Affirming Medical Care. GAMC Statement. https://www.gamcstatement.org/
[105] Michaels, S. (2016, April 25). We tracked down the lawyers behind the recent wave of anti-trans bathroom bills. Mother Jones. https://www.motherjones.com/politics/2016/04/alliance-defending-freedom-lobbies-anti-lgbt-bathroom-bills/
[106] Hart (2017)
[107] Detta, N. (2021). Tip of the Iceberg: Religious Extremist Funders against Human Rights for Sexuality and Reproductive Health in Europe 2009 - 2018. European Parliamentary Forum for Sexual and Reproductive Rights. https://www.epfweb.org/node/837. See also Namubiru, L. (2023, July 5). Charity loophole lets US donors give far-right groups $272m in secret. openDemocracy. https://www.opendemocracy.net/en/5050/donor-advised-funds-daf-us-charity-law-loophole-bankroll-hate
[108] Amend, A. (2017, July 27). Anti-LGBT Hate Group Alliance Defending Freedom Defended State-Enforced Sterilization for Transgender Europeans. Southern Poverty Law Center. https://www.splcenter.org/hatewatch/2017/07/27/anti-lgbt-hate-group-alliance-defending-freedom-defended-state-enforced-sterilization
[109] Genspect. (n.d.). The Killarney Group Think Tank. Genspect. Retrieved October 16, 2023, from https://web.archive.org/web/20231017000902/https://genspect.org/meet-the-team/the-killarney-group-think-tank/
[110] See Genspect. (2023, March 3). Genspect Goes for “The Bigger Picture.” Genspect. https://web.archive.org/web/20230314215125/https://genspect.org/genspect-goes-for-the-bigger-picture/; Jones, Z. (2023, October 1). SEGM conference flier revealed: Invited speakers and schedule for October 9-12 New York City conference of the anti-trans Society for Evidence-Based Medicine. Gender Analysis. https://genderanalysis.net/2023/10/segm-conference-flier-revealed-invited-speakers-and-schedule-for-october-9-12-new-york-city-conference-of-the-anti-trans-society-for-evidence-based-medicine/
[111] Ayad, S., D’Angelo, R., Kenny, D. T., Levine, S. B., Marchiano, L., & O’Malley, S. (2022). A Clinical Guide for Therapists Working with Gender-Questioning Youth. Gender Exploratory Therapy Association. https://web.archive.org/web/20230106171127/https://genderexploratory.com/wp-content/uploads/2022/12/GETA_ClinicalGuide_2022v1.1.pdf. The authors of the guide state “We would like to thank the Society for Evidence-Based Gender Medicine for their support in the creation and production of this guide.”
[112] Genspect. (2023, June 16). Genspect Launches New Think Tank to Draft a Gender Care Framework. Genspect. https://web.archive.org/web/20231017001201/https://genspect.org/genspect-launches-new-think-tank-to-draft-a-gender-care-framework/
[113] Piper (2023)